



Retinoid Toxicity
Why do I care?
As a dietitian I have sworn by carrots as a health promoting anti-cancer food and then I learned of Retinoid Toxicity as a possible causal factor of chronic fatigue, skin rash and other symptoms. I cut out carotenoids and vitamin A and started feeling much better for the first time like in ever. I may have been over-activating vitamin A to Retinoic acid since birth, or childhood vaccines, or teen years Epstein-Barr virus. It just helped to find out that not eating carrots, kale, sweet potatoes, peaches, or fortified foods would help me feel better.
As a dietitian I also no longer feel comfortable flatly saying that carotenoids are safe and good for everyone - because there may be many other people who might find out with an elimination diet that they also feel better without having carrots, liver or vitamin A fortified milk/equivalent beverages in their diet.
*Near email length, but this is a page? I am going to pause here with the note that this is a complex topic and more How-to’s are needed for an elimination diet - simply though, cut out almost all rich carotenoid foods and processed foods that use them as an ingredient (tomato and carrot are in most canned soups), and meats and dairy may need to be removed too. Follow a strict removal for a few weeks at least to give the body time to heal, and then if it isn’t obvious that it helped retry a vitamin A food and see if negative symptoms return the next day after eating it. On the same day there may be improved feelings, but that can be temporary until the liver changes the vitamin A into active Retinoic Acid which causes many inflammatory events to start.
What is Retinoid Toxicity?
Retinoid Toxicity refers to a set of negative symptoms caused by excess active vitamin A. Short term it can feel flu-like symptoms as activated vitamin A is heavily involved in our immune response. Excess of the active form will make the body think there is an infection to fight. Puffy edema, congestion, pain, skin rashes, sun sensitivity, and fatigue may be present. Over time, long term excess active Retinoids can lead to liver, kidney and/or brain damage, occurring as a result of the chronically inflamed body.
Vitamin A in the inactive form is needed within rhodopsin to sense light and in the active form is hormone like and involved in gene transcription of tens of thousands of genes either directly or indirectly by effects on other receptors involved in gene transcription such as the thyroid and Vitamin D receptors.
Symptoms of Retinoid Toxicity
Symptoms of excess active vitamin A chronically may include:
“The most common side effects of chronic vitamin A toxicity — often referred to as hypervitaminosis A — are,(4):
vision disturbances
confusion
sunlight sensitivity
dry skin [&/or chapped lips, with non-healing sores at the corners of the lips]
itchy skin
hair loss
decreased appetite
nausea and vomiting
delayed growth [children with hypervitaminosis A may be stunted, shorter than their potential, (6)]
joint and bone pain
liver damage
jaundice. (4)
The symptoms would vary with severity of the excess intake and duration of use. Excess Retinoic acid is a serious problem that is likely not being recognized and instead is being called a variety of conditions with other labels. See the post: Houston we have a problem for reference (4) and (6) and see my Table 1 Symptoms of Histamine Excess and Retinoid Toxicity, (pdf in my Dropbox), for more detail with research references.
I wrote a self-evaluation survey for symptoms: Retinoid Toxicity Symptom Questionnaire - by Jenny (substack.com)
Who may have excess active Vitamin A as an underlying factor in their chronic health symptoms?
Typically, Retinoid Toxicity has been associated with Retinoid medications used for acne, skin treatments and in cancer care. Stopping the medication is the usual ‘treatment’ or reducing the dosage and the symptoms resolve.
Many other chronic conditions may have excess active Retinoids as a causal factor for the symptoms - and therefore any treatment that is attempted will only be a bucket of water trying to put out a forest fire. We need to stop the forest fire that the excess active vitamin A causes. It is designed to fight an infection - which may need a forest fire equivalent of white blood cells, cytokines, and degranulated mast cell histamine. But we don’t need that every day if there is no longer an infection.
Recent theories suggest Retinoid Toxicity is involved in the symptoms of conditions following viral infection such as ME/CFS and in the traditionally vaccine injured, and other cases with liver injury (Mawson, Croft, 2020) which may be leading to excess active retinoids being released - possibly those who develop symptoms of akathisia/drug side effects after pharma use or withdrawal.
Over activation of vitamin A or carotenoids to Retinoic acid may become a lifelong problem after prenatal alcohol exposure, or immune challenge from certain viral infections (Epstein Barr Virus: (Jones, R.J., et al, 2007) and possibly SARS-CoV-2: (Bonilla, et al, 2022; Mawson et al, 2021). Vaccine injury and other drug related chronic symptoms including akathisia may also be related to retinoid excess related to liver injury. (Mawson, Croft, 2020)
In ME/CFS a gene change that may help Epstein-Barr virus infect mature epithelial cells. The active Retinoic Acid promotes differentiation of epithelial cells to the mature form. (Jones, R.J., et al, 2007) A similar effect may be occurring with SARS-CoV-2 with differentiation and infection of endothelial cells.
Who may be affected by Retinoid Toxicity?
Myalgic Encephalo-Myelitis/Chronic Fatigue Syndrome, (ME/CFS):
Fibromyalgia
Mast Cell Activation Syndrome, (MCAS)
Alcoholics and possibly children of males (ADHD) or females (FAS) who drank prior or during the prenatal development of the infant.
People taking retinoid medications and/or high dose supplements of vitamin A and/or eating a lot of foods rich in vitamin A such as liver.
People with liver injury or pharma drug reactions of akathisia developing during use or withdrawal of the medication/s.
1. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
The cause of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is not well understood but has been linked to prior viral infection with “Epstein-Barr Virus (EBV), Human Herpesvirus (HHV)-6, and Human Parvovirus B19. [23,24,25,26,27,28,29]”. (CC-BY the authors Varesi, et al, 2021) Gut dysbiosis is suggested as a treatment approach by Varesi, et al., based on the frequent comorbidity of inflammatory bowel conditions with ME/CFS. (Varesi, et al, 2021)
Increased inflammation and reduced mitochondrial function are seen in ME/CFS:
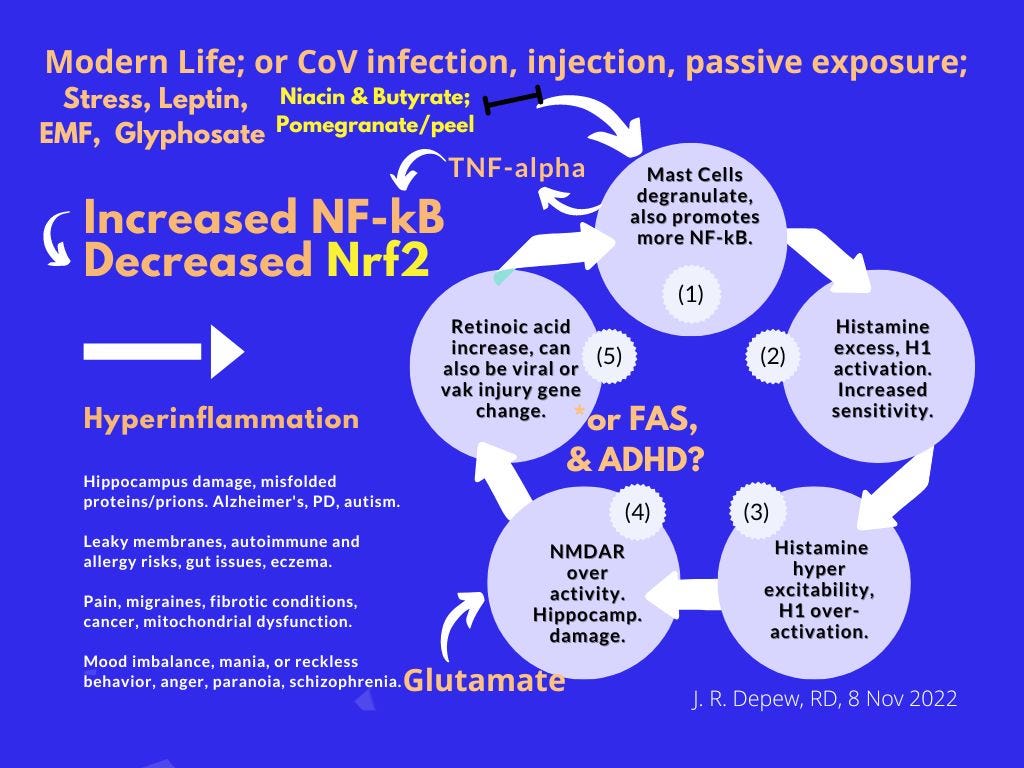
Key mechanisms in ME/CFS are increased levels of inflammatory cytokines and NF-κB and decreased p53, mitochondrial dysfunction with lowered ATP production. This would provide an explanation for typical symptoms of ME/CFS of fatigue, pain, and post-exertional malaise, and the neurologic and autonomic symptoms. The decrease in p53 activity leads to more anaerobic glycolysis in the mitochondria, which increases lactate levels, reduces numbers of mitochondria in skeletal muscle and reduces endurance. The increase in NF-κB leads to more reactive oxygen species and pro-inflammatory cytokines, which further compromises mitochondrial function and promotes anaerobic glycolysis. (Morris and Maes, 2012)
Epstein-Barr Virus seems to be involved in ME/CFS and may be reactivated after a SARS-CoV-2 infection:
Plasma and saliva samples from non-vaccinated ME/CFS (n=95) and from healthy donors (HD)(n=110) were analyzed using soluble multiplex immunoassay for anti-SARS-CoV-2 antibodies. Anti-viral antibody fingerprints in saliva were used to detect reactivation of human endogenous retrovirus K (HERV-K) and human herpesviruses 1-6 (HSV1, HSV2, VZV, EBV, CMV, HHV6). Virus-specific antibodies for latent viruses were identified 3-6 months after an infection with SARS-CoV-2 in patients with ME/CFS. The antibody responses were stronger in the patients with ME/CFS and particularly to the EBV-encoded nuclear antigen-1 (EBNA1). ME/CFS patients also had elevated IgG which was not observed in the control group (HD). At baseline prior to SARS-infection, the ME/CFS group had elevated EBV-VCA IgG unlike the HD group. (Apostolou, et al., 2022)
2. Fibromyalgia
Fibromyalgia involves fatigue and widespread pain but the cause is unknown. Patients with fibromyalgia are described as being more sensitive to pain by the CDC webpage, they instead may be experiencing more pain than normal, and throughout the body simultaneously. (cdc.gov/Fibromyalgia) Acute retinoic acid toxicity symptoms felt similar to fibromyalgia for me (n =1) for a day or two after accidentally eating ¼ of a peach.
Females are more likely to have fibromyalgia and may be more sensitive to pain than males due to TRP channels that have a narrower sensitivity range. Males needed four times more capsaicin (TRPV1 activator) on average than females to have a similar reaction. (Lu et al, 2009 as cited by Artero-Morales, et al, 2018)
3. Mast Cell Activation Syndrome (MCAS)
MCAS involves histamine excess due to overactive mast cell degranulation, and retinoic acid can degranulate mast cells. A person with MCAS may not have Retinoid Toxicity problems, but a person with Retinoid Toxicity problems will also likely have symptoms of histamine excess and overactivation of mast cells. So therapeutic diet and lifestyle changes are similar.
MCAS leads to increasing sensitivity to trigger foods, with more limits and to smaller amounts as sensitivity increase. Also changes in temperatures - summer heat to chilly indoor air conditioning - can be a trigger which suggests TRP channels are involved. Increased expression of TRP channels has been observed in inflammatory bowel conditions. (Hicks, 2006, González-Ramírez , et al, 2017) Excess bradykinin or serotonin can increase sensitivity of channels. (Horvath, et al, 2016; Morita, et al, 2015)
Exercise increases inflammatory myokines – a moderate pace is important for histamine excess sufferers. See: Table 3 – Self-care Guidance. Vitamin D adequacy would reduce risk for increasing food allergens or autoimmune antibodies to molecular mimicry proteins. See: Table 2– Potentially Inflammatory Foods and Table 5– Nutrients. *The Tables aren’t my most recent drafts or numbers but are in my Dropbox on single pages already.
Triggers and symptoms of MCAS are varied and fluctuate – episodic. This makes it hard for patients to identify their problem foods or lifestyle events and severity tends to increase with time. Triggers may include stress, exercise, perfumed items, and changes in temperature. (mastcellaction.org/about-mcas) I would add flickering or strobe light effects as a trigger also. Action movies, concerts, night-time driving, may all cause a histamine excess induced migraine the next day.
Being sensitive to changes in temperature would indicate a TRP channel over-activation problem – and the long-term solution is to reduce inflammation and dress in layers. Prevent TRP activation by adding or removing a sweater as the internal thermostat sensors became over-sensitive to getting too hot or cold. (Table 3 – Self-care Guidance)
Low Histamine Diet food guidance is in this document: Histamine Food Lists (pdf in my Dropbox), and on the MCAS/Histamine page of jenniferdepew.com. The pdf also has the Nrf2 promoting phytonutrient graphics, other inflammatory issues and discusses Retinoic Toxicity.
Alkalizing Foods that may help, other inflammatory food issues that may not. TRP channel activators, Lectin, Oxalates, Retinoic Acid, Histamine (pdf in my Dropbox) has food lists showing what is more acid producing after digestion and what foods are more alkalizing - and likely more beneficial. Cancer and mitochondrial dysfunction are associated with more acidic body fluids. That pdf also has more detail about other inflammatory groups of foods/chemicals in foods - oxalates, lectins, TRP channel activators, and links to Histamine and Retinoic Toxicity information.
The Basic stack, melatonin, niacin, and glyphosate graphics and Nrf2 promotors are included in the Alkalizing Foods document. Those graphics are discussed in more detail, with guidance about modifying doses for children on the page Prenatal/Child, jenniferdepew.com.
Beans are an alkalizing food that also may help with detox of toxins and protect the liver. See the post: Beans for breast cancer? and liver health?
Symptoms of Retinoid Toxicity and Histamine Excess overlap a lot, and both can lead to kidney, liver and/or brain damage over time. Symptoms can vary a lot and tend to be called other names diagnostically and treated in ways that generally don’t address the histamine and/or active Retinoid excess. Although antihistamines are used for some mental health and other conditions that wouldn’t seem to warrant an “allergy” drug.
4. Alcoholism and paternal or maternal alcohol use.
Gene changes causing excess activation of vitamin A may also be caused by alcohol use and effect the drinker and potentially their offspring. Male alcohol use is linked to ADHD - like Fetal Alcohol Syndrome that is not affecting the baby as visibly as when a pregnant woman is using alcohol too. The DNA of the sperm can become damaged, creating alleles that may cause dysfunction of the protein it encodes. Alcohol use causes over-activation of vitamin A to active Retinoids within the liver and the active form is transported out of the liver to the rest of the body. This also leads to a depletion of inactive vitamin A and night blindness is common in chronic alcohol drinkers.
It takes 74 days to grow a sperm - how many days out of 74 do some people drink alcohol?
A) None. B) All of them. C) Weekends, heavy use, (one Fifth/day = 17 beer equivalents. D) Weekends, light use. E) One glass of wine every evening. F) One six pack every evening. G) One pint every evening (~8.5 beer equiv). H) 3-4 days a week, a wine cooler/beer/wine/shot. I) 3-4 days a week, (3-4) several beers or a mixed drink with a few shots. J)* 1-2 days a week, 1-2 servings. K)* 1-2 days a week, 3-4 servings. {*these answers are similar to D)} L) 1-2 drinks per month. M) Heavy use once a month. N) All of the Above.
Reference: Standard Alcohol Serving Sizes equivalents, (uwm.edu).
The correct answer to the question as I phrased it is “N) All of the Above.” People have different ideas about what normal drinking might look like. Standard questionnaires may not get a full picture of a person’s risk. Choice “E) One glass of wine every evening” is likely less risk than the “C) Weekends, heavy use,” whether it is a six-pack, a pint or a fifth a day. Drinkers can drink a lot of alcohol. But on a questionnaire one person may have to write “drinks 7 days/week” and the other might respond “drinks 2 days/week” and seem like less of a problem drinker than the one glass of wine with dinner person (a European pattern).
If trying to be healthier for body, brain, and sperm: Less risky patterns are the A), E), H), J), L), and K) is slightly more but not too bad. I) is moving into being a ‘drinker’ but not yet a ‘problem drinker’ - it is probably enough to be a negative on DNA methylation and damage repair. Have extra B vitamins, C, and magnesium and potassium foods to help the body clear alcohol out. Avoiding excess vitamin A foods and carotenoids might be helpful but more of a need for a chronic drinker {B), C), F), G)}
Two servings/day is a moderate recommendation for males/larger build, and one serving/day is the recommendation for females/smaller build. Some ethnic groups do not detox alcohol well and would be better off abstaining or having small servings. Healthy benefits of alcohol can be seen with a third of the typical serving size - the medicinal half shot of whiskey after a shock or a two-ounce taster of wine.
5. People taking retinoid medications, high dose vitamin A supplements, or rich food sources routinely.
Retinoid medications are used for acne or anti-aging skin products and for some types of cancer. If toxicity symptoms occur generally the medication is stopped or reduced.
See: Retinoic Acid and Toxicity dosing - How much (liver for example) is too much?
6. People with vaccine or liver injury or pharma adverse reactions like akathisia.
Liver injury may be involved in chronic symptoms following traditional vaccines and in other cases with liver injury as active retinoids may be released in excess. (Mawson, Croft, 2020)
See this post with the initial draft of my pomegranate paper for more information about the link between ME/CFS and retinoid toxicity:
Pomegranate, TRP channels, nociceptive pain, butyrate and endocannabinoids. (substack.com) *I started over on the second draft which is more about nociceptive pain and other topics and less about ME/CFS and retinoid toxicity.
Other resources mentioned earlier: See the post: Houston we have a problem and my Table 1 Symptoms of Histamine Excess and Retinoid Toxicity, (pdf in my Dropbox), for more detail with research references.
I wrote a self-evaluation survey for symptoms: Retinoid Toxicity Symptom Questionnaire, (substack.com).
Disclaimer: This information is being shared for educational purposes within the guidelines of Fair Use and is not intended to provide individual health guidance.