

My research paper, initial progress
*Needs more Tables and Figures and References added, and the evidence in more detail. Still working on it.

Pomegranate phytonutrients for mast cell inhibition to reduce the pain and suicide risk associated with histamine excess in neurologic conditions, drug related akathisia or post infection illness.
Abstract
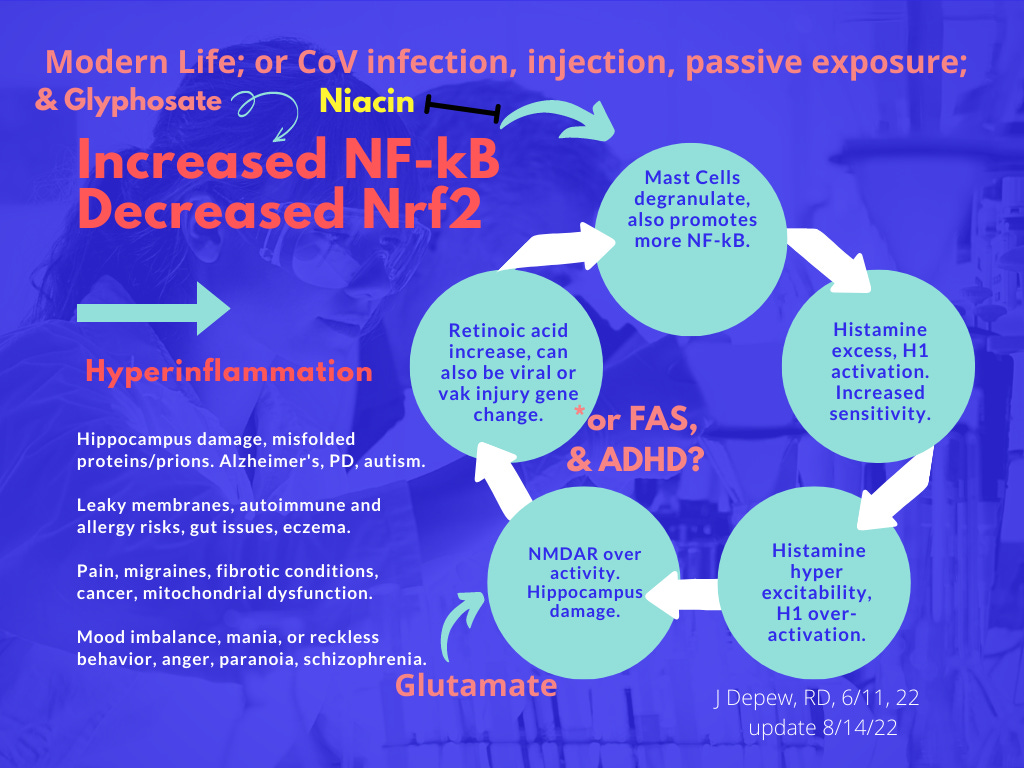
Problem – Retinoic acid deficiency or excess and histamine excess are seen in many neurological conditions including schizoaffective disorders, FAS, ADHD, autism spectrum disorder and Alzheimer’s dementia; and in ME/CFS following Epstein-Barr Virus. ME/CFS has been seen in Covid19 survivors. Attempts to use histamine antagonists or reverse agonists for symptoms of histamine excess have had limited success due to adverse effects from peripheral Histamine receptors. (Cheng et al, 2021) Use of vitamin A or retinoids has also had mixed results. Evaluating why individuals have excess histamine is needed. Then targeted care could be provided to reduce the degranulation of mast cells and release of histamine or mitigate for other genetic differences affecting retinoid metabolism or the histaminergic system that can lead to a tendency towards histamine excess, which can then lead to hippocampal damage over time. NMDA receptor antagonists can be protective in addition to antihistamine medications. Instead of the side effect risk of histamine receptor antagonists, reducing the level of histamine could provide improved quality of life and reduce the mental and physical pain of excess histamine levels – which can range from seasonal allergies and migraines to emotional dysregulation with risky behavior or severe anxiety, to suicidal urges and self-harm.
Acute symptom management solution – Polyphenols in pomegranate fruit or peel, and other produce with quercetin and luteolin, can reduce the histamine symptoms within a short time frame by inhibiting mast cells or modulating the inflammatory cytokines that are also released. Having a two to three-ounce serving of pomegranate juice or seeds twice a day can be inconvenient and expensive. Treatments made with the more potent peel can be produced inexpensively for year around use (seasonal fruit). The tannin content of the outer peel is a factor that adds diuretic effects, which is helpful for detoxification but may limit medicinal use except as an extract or for use in milligram amounts. Pomegranate products also promote microbiome health and improve symptoms of Metabolic Syndrome. Postbiotic metabolites may be formed from pomegranate phytonutrients that can cross the blood brain barrier, reduce neuroinflammation and may promote regrowth of hippocampal cells. Mineral chelation properties promote antimicrobial and anticancer effects (with reduction of metastasis risk in particular) and chelation of other toxins and adsorption of nanoparticles.
Introduction
Histamine excess and/or retinoic acid excess may be causal in many neurological conditions (Fernández-Novoa et al, 1994) including schizoaffective disorders, FAS, ADHD, autism spectrum disorder and Alzheimer’s Dementia. It can cause pain ranging from seasonal allergies to severe mental illness – histamine hyperexcitability with emotional dysregulation. Self-injury, panic, anxiety, suicidal urges, or mania and reckless behavior can occur and may be diagnosed as schizophrenia or bipolar disorder Type 1 and be treated with psychiatric medications that would not reduce histamine levels.
Histamine excess can cause severe mental symptoms that may include suicidal urges – daily if the excess histamine levels are present daily. Suicide is a risk in schizophrenia yet other chronic damage on average causes death more often in the cohort. The histamine excess causes inflammatory symptoms throughout the body and targets the hippocampus which may lead to an Alzheimer’s diagnosis later in life. Histamine functions as a neuromodulator, excess leads to hyper-escalation of brain activity and mood whether anxious fear or manic grandiosity, which leads to an increase in mitochondrial workload and oxidative stress chemicals. Extra antioxidants and cofactors would be needed or worsening of mental health symptoms is likely as nutrient deficiencies become severe.
Histamine excess is debilitating physically and mentally, and chronically can lead to hippocampal damage and Alzheimer’s dementia.
Histaminergic abnormalities or histamine excess are seen in many neurologic conditions.
Pain may vary from minor seasonal allergies and inflammation to more severe mental psychosis and self-injurious behavior or suicide risks.
Current treatment use of antihistamines or reverse agonists for narcolepsy have had side effects of sleepiness or peripheral histamine receptor side effects. (Cheng et al, 2021)
Currently diagnosis of histamine excess problems may be inconclusive, yet the problem may be ruled out based on the lab tests for DOA enzyme or histamine levels.
More effective screening and treatment methods are needed for acute treatment during histamine excess and for prevention over time.
The problem of histamine excess is multi-factorial with varied potential causal factors which would need targeted treatment specific for each individual or group with a similar cluster of causal risks. Thorough screening would be needed to identify genetic differences affecting digestion or metabolic pathways, nutrient imbalance, and lifestyle variables that may affect mast cells or stress. Varied treatments would then be needed to mitigate for each of the identified potential causal factors. Treating only one or a few might leave enough causal issues that symptoms remain. Gradually working through a list might make it possible to eventually restore optimal function and improve the patient’s quality of life – as long as the improvements continue on a daily or frequent enough basis to prevent a return of histamine excess in the diet, or nutrient imbalances, or excessive mast cell degranulation – or all three.
The diagnostic tests for histamine excess or mast cell over activation can be inconclusive. Retinoic acid levels may need to be checked in specific tissue locations as the over activation may be localized. In chronic alcoholism the liver over activates Retinoic acid and transports it elsewhere in the body leading to deficiency levels in the eyes and liver and excess in the testes* (*drinking by males prior to conception is a link between FAS and ADHD) and elsewhere. Less is known about over-activation continuing after a viral infection (EBV (Jones, et al, 2007), possibly SARS-CoV-2 (Bonilla, et al, 2022)) and causing the varied symptoms of ME/CFS.
Over activation of vitamin A or carotenoids to Retinoic acid may become a lifelong problem after prenatal alcohol exposure, or immune challenge from certain viral infections (Epstein Barr Virus (Jones, et al, 2007) and possibly SARS-CoV-2 (Bonilla, et al, 2022)).
Retinoic acid excess would cause mast cell degranulation and increase histamine. It can lead to liver and kidney damage in addition to neurocognitive degeneration risks and other chronic pain symptoms of seasonal allergies, migraines, skin rashes, bone spurs, and inflammation. Histamine excess may then be more of a risk and intermittently possibly based on varying intake of vitamin A rich meals or supplements or topical products. Histamine hyperexcitability might then also be intermittent with extreme fear or mania happening due to liver dinner and peach cobbler the day before. Pomegranate polyphenols might help during the episode but knowing to avoid vitamin A and histamine foods in the first place would be better.
Causal factors for histamine excess seen in neurological conditions may include:
Heterogeneity of metabolic gene alleles that leads to a similar phenotype of histamine excess.
Low methylation or a difference in the DOA enzyme might be causal factors treated with methylated forms of folate and B12 and choline, or supplements of the enzyme DOA which breaks down histamine.
Other gene differences might decrease ability to reduce oxidative stress and the resulting inflammation risk could lead to more degranulation of mast cells and release of histamine.
Endocannabinoid deficiency or imbalance due to genetic differences can be causal as both the THC and CBD equivalents, anandamide and 2-AG, are needed to inhibit a mast cell from degranulating. (BHMT gene is an example).
Retinoic acid, the active form of vitamin A, is involved in immune function and can cause degranulation of mast cells and add to an histamine excess problem. Over activation of vitamin A or carotenoids to Retinoic acid may be a gene difference that can result from Fetal Alcohol exposure from the sperm arriving with alcoholic DNA damage, or prenatal alcohol use. Alcohol use in an adult affects retinoic acid activation leading to low levels being present in the liver and eyes and increased transport from the liver to other areas of the body including the testes.
Vaccine injury; certain viral infections (Epstein-Barr virus (EBV) (Jones, et al, 2007) and SARS-CoV-2 has led to similar ME/CFS problems as seen in EBV survivors, (Bonilla, et al, 2022)); and possibly the drug reaction referred to as akathisia (~restless legs, but it can include mental symptoms), may also lead to an ongoing increase in the liver activation of carotenoids or vitamin A to the active Retinoic Acid form due to genetic changes. From the liver the activated Retinoic Acid is sent out to the body on transport proteins.
Diet related factors:
Diet is a source of histamine. Reducing use of histamine food sources or foods that increase mast cell activation in the gut may make a very significant improvement in symptoms.
If Retinoic Acid overactivation was found to be a problem, then strictly reducing vitamin A and carotenoids in the diet may also be needed for significant improvement to be seen.
Glyphosate increases inflammatory Nf-kB which reduces anti-inflammatory Nrf2 and adds to the degranulation of mast cells.
Other lifestyle or trauma history factors:
Circadian cycle abnormalities; EMF; flickering lights/strobe light like effects in media; and stress whether physical or emotional; also can cause degranulation of mast cells and may lead to a migraine the morning after an increase in exposure (went to see an action movie last night). Wearing dark sunglasses can protect against the flickering light trigger.
Psychosomatic symptoms or trauma history may be a factor as emotional or physical stress can add to the mast cell activation. (Baldwin, 2006) In schizophrenia psychosomatic symptoms were not found to be that common which was taken to suggest that there is a biologic basis to the condition. Identifying and working through any emotionally caused symptoms may be needed in addition to other strategies in order to restore optimal quality of life as the emotional pain could be adding to histamine excess too, due to the degranulation of mast cells. (Baldwin, 2006)
Causal factors for excess histamine or Retinoic Acid can include, summarized:
The average diet is high in histamine foods, so intake is daily for most people – but not everyone has excess histamine problems. Sensitive people may have methylation gene alleles leading to low folate and poor breakdown of histamine,
Or a gene allele causing dysfunction of the DOA enzyme that breaks down histamine.
Prenatal alcohol exposure, FAS (maternal use), ADHD (paternal use) potentially may leave the liver over-activating Retinoic Acid (RA).
Chronic Alcoholism causes over-activation of RA while leaving the body low in the inactive form of vitamin A.
Epstein-Barr Virus (EBV) (Jones, et al, 2007), or possibly SARS-CoV-2 infection (Bonilla, et al, 2022), may cause ongoing over-activation of RA by the liver leading to symptoms diagnosed as ME/CFS.
Vaccine injury and possibly drug injury (more research is needed) may also.
Retinoid medication or supplement toxicity – this is currently the only well studied cause of Retinoid toxicity.
Other nutrient or cofactor deficiencies may also be causal factors to treat with supplements and/or diet changes; Niacin, tryptophan, magnesium, iodine, Acetyl carnitine, N-acetyl cysteine, Nrf2 promoting phytonutrients which include pomegranate products - Mitochondrial support nutrients.
Emotional or physical stressors may also increase histamine. (Baldwin, 2006)
Flickering or strobe lights can cause degranulation of mast cells.
Glyphosate or other unknown contaminants may be inflammatory or inhibiting metabolic pathways.
The summaries above are likely not all inconclusive but begin to show the complexity of potential causal factors for histamine excess and/or Retinoic Acid excess. Antihistamine medications can help dampen some flames of excess histamine but blocking receptors will not stop the influx of more histamine from dietary sources, or histamine that lifestyle and stress may be adding each day from mast cell degranulation.
Polyphenols from pomegranate and other produce sources of quercetin or luteolin can help inhibit the mast cells and reduce symptoms of histamine excess. Pomegranate peel extract was found to inhibit NF-kB, (Rasheed, et al, 2009), which makes sense as it is an Nrf2 promoter. Field tests suggest 3-4 ounces of juice or seeds can be calming within 20 minutes, and pomegranate peel foods also help but digestion may slow down the calming response (Personal experience, n=2). Nrf2 promoting herbs and mitochondrial support nutrients can help reduce inflammation that leads to more mast cell degranulation. Using methyl folate and avoiding histamine foods or trigger foods can help prevent the excess accumulation of histamine from the gut. More controversially, inhaled THC and CBD, in combination, also inhibits mast cells from degranulating.
Discussion: Multifactorial problems require multifactorial solutions.
Self-care is not easy in a busy world, and it is more difficult with mental health problems or physical pain and fatigue. Patients suffering from such a varied and complex problem will need a complex solution that would be challenging for a dietitian (*lived experience, n=1) to cope with. Mixed histamine reducing herbal products are available on the market. Adding pomegranate peel extract or urolithin A or B (gut metabolite of pomegranate) to a mixed product with mitochondrial support nutrients, Hawthorne, Nettle, or other herbs, might help provide patients, staff, parents and individuals with a calming strategy. Reducing the severity of mental symptoms of histamine excess might help restore enough function to be able to work on other lifestyle and dietary factors that might be adding to an individual’s symptoms.
Screening with lab tests might be misleading compared to a Therapeutic Trial – does a serving of pomegranate, quercetin, or luteolin help calm a patient’s symptoms? Elimination diets are also helpful to see if diet is a causal factor and would also be a Therapeutic Trial of the recommended diet. If it works – just continue. Would following a low histamine diet for a month lead to a reduction in symptoms? If not, would restricting vitamin A and carotenoid foods help more?
Screening questionnaires may be helpful as the list of histamine excess symptoms and Retinoid Toxicity symptoms are not the same and both include some unusual symptoms, other than congestion, fatigue, and edema. Endocannabinoid deficiency generates a third list of potential symptoms or diagnoses frequently associated with lack of cannabinoids or imbalance (schizophrenia).
Resources for cognitive therapy techniques are included in the Tables as the danger to the patient during histamine excess can be severe and immediate coping skills can be life-saving during impulsive and irrational moments. Practice and having a plan discussed with a trusted authority can be the most necessary tool at a time of need and then the bottle of calming pomegranate may be a second step.
~~~~~~~
Table 1. Symptoms of histamine excess and symptoms of Retinoid Toxicity are very similar.
*Imagine this as a Table. Hyperinflammation can lead to cell death.
Histamine Excess: Increased IL-6 and NF-kB. (Park, et al, 2014) Cell death can occur.
Retinoid Toxicity: Vitamin A deficiency increases NF-kB. Activated Retinoic Acid can reduce NF-kB and IL-6 levels. (Austenaa et al, 2004) Inflammation will lead to depletion of retinol as it is converted to Retinoic Acid and deficiency will then increase inflammation more. (Sarohan et al, 2021) Cell death can occur. (De Oliveira, 2015)
Skin and Bone effects of Histamine Excess and Retinoid Toxicity.
Skin, Histamine Excess: Rash in histamine excess tends towards hives. Skin reddening very easily and staying red briefly – being able to write on your with your fingernail can occur in histamine excess.
Skin, Retinoid Toxicity: “Mucocutaneous effects include dry lips, cheilitis, and dry oral, ophthalmic, and nasal mucosa. The putative mechanism is decreased sebum production, reduced epidermal thickness, and altered barrier function. Other cutaneous effects seen include overall skin dryness and pruritus, peeling of palms and soles, and fingertip fissuring. Telogen effluvium may be seen with higher doses.” (Olson et al, 2020) Telogen effluvium is hair loss and thinning without scarring, the problem may be acute or chronic. (10)
Bone, Histamine excess: Histamine increases inflammation in osteoarthritis. (Wang et al, 2019)
Bone, Retinoid Toxicity: Bone spurs, calcinosis, and hypercalcemia. (Scheven, Hamilton, 1990) Risk of osteoporosis and hip fractures. (Genaro Martini, 2004) (Olson et al, 2020)
Metabolism - thyroid and blood lipid, sugar, and weight effects.
Hypothyroidism, Histamine excess: Hypothyroidism may increase expression of mast cells & histamine risk, or MCAS may affect thyroid functions. (Landucci, et al, 2019)
Hypothyroidism, Retinoid Toxicity: Hypothyroidism. (Sherman, et al, 1999) (Olson et al, 2020)
Blood chemistry, histamine excess: Histamine is involved in blood lipids, glucose, insulin, and weight. (Masaki et al, 2001)
Blood chemistry, Retinoid Toxicity: Hypertriglyceridemia and other blood lipid changes, (Koo, et al, 1997) (Duvic, et al, 2001) Rare – also acute hemorrhagic pancreatitis and eruptive xanthomas. (Olson et al, 2020)
Liver damage.
Hepatic dysfunction, Histamine Excess: Hepatomegaly, fibrosis. (Yam et al, 1986) Either excess or too few mast cells in the liver can lead to fibrotic damage. (Jarido et al, 2017)
Hepatic dysfunction, Retinoid Toxicity: Elevated serum transaminases and liver damage leading to fibrosis and hepatic stellate cell activation. (Nollevaux, et al, 2006) (Olson et al, 2020)
Kidney damage.
Renal Dysfunction, Histamine Excess: Renal dysfunction. See Fig 3. Acute Kidney Injury, diabetes, and hypertension. (Sudarikova et al, 2021)
Renal Dysfunction, Retinoid Toxicity: Renal dysfunction. (Cribier, et al, 1992) (Olson et al, 2020)
Neurological symptoms.
Headaches, Histamine Excess: Migraines may be frequent and severe. (Personal experience.)
Headaches, Retinoid Toxicity: Headache, nausea, and vomiting; rare -pseudotumor cerebri syndrome. (Chisholm, et al, 2018) (Olson et al, 2020)
Anxiety/other, Histamine Excess: Extreme anxiety, fear, suicidal ideation, mania, hyperexcitability. (Personal experience/citations needed)
Anxiety other, Retinoid Toxicity: Possible link: depression, psychosis, or suicide attempts. (Bigby, 2008) (Olson et al, 2020) “Confusion, irritability, anxiety, depression, and suicide ideation.” (Snodgrass, 1992) Schizophrenia like ‘hysteria’ after eating polar bear liver. (Rodahl, Moore, 1943) (Restak, 1972) (De Oliveira, 2015)
Dopamine imbalance, Histamine Excess: Dopamine & ROS levels would be elevated during histamine excess and hyperexcitability episodes.
Dopamine imbalance, Retinoid Toxicity: Effects on neuronal function may include: “impaired bioenergetic parameters related to mitochondrial function, oxidative and nitrosative stress, alterations of dopamine signaling, and behavioral disturbances.” (De Oliveira, 2015)
Lab measurements that might be informative.
Histamine Excess: “In humans, although the plasma histamine levels were low (< 1 ng/mL) in normal conditions, 17 out of 54 patients with atopic eczema showed plasma histamine concentrations ranging between 1.2 and 5.2 ng/mL.7” ((Ubuku 2021) viewable at ScienceDirect)
Vitamin A Toxicity - Retinol in the liver: Normal level of Vit A in the liver (1H-retinol) “is about 100 µg/g (Furr et al. 1989). […] roughly 300 µg/g in the liver reveals intoxication (Olson 1993). ” (De Oliveira, 2015) Measurements of retinoids and retinol may vary in different parts of the body. Retinol is low in the alcoholic liver and eyes, leading to night blindness, while other areas of the alcoholic person’s body has excess Retinoic Acid. The gene change seen in Epstein Barr Virus ME/CFS patients may also lead to the liver showing low levels of retinol while the rest of the body may be experiencing elevated amounts of the activated forms of Retinoic Acid.
~~~~~~~~~
There seems to be a pattern in the table above (the imaginary table).

Table 2: Counseling Strategies for Coping with Urges to Self-Harm.
Substitution or Distraction Strategies. Once a trauma pattern is in place, substitution to replace the learned pattern is needed, the habitual actions will be repeated when under stress. Turn a hitting pattern into a hair brushing pattern, perhaps.
Substitute less harmful actions. When self-injury is already occurring, starting with a substitution behavior that represents the typical method used to self-harm may be needed rather than will-power. For example, drawing a red mark instead of cutting, pounding a pillow instead of hitting oneself.
Breathing techniques. We tend to hold our breath in stressful situations and lack of oxygen makes rational thinking and self-control more difficult.
Creative Visualization. Visualize a happy place or memory or some other practiced calming scenario to help distract from or replace negative thought patterns.
Exercise; walk, dance, jog, yoga. Release tension with real exercise instead of mental or physical pain. Caution that a stress cleaning habit doesn’t become self-harm too.
Write about worries or write creatively. Journaling about what you are grateful for can help to see that life is worth it even though difficult too. Journaling about worries can help work through to solutions or seeing it isn’t that bad.
Create art. Early childhood trauma may be non-verbal and art in many forms can help work out those unspoken memories or feelings.
Enjoy music. Creating music can also release nonverbal feelings. Caution: frequencies and rhythms can be healing to the body rhythms or unsettling, recognize and turn off music if it makes you more upset.
Talk it out. Humans are social and benefit from connections with others. Phone a friend, counselor, or hotline or make a private audio journal. Some people blog or vlog, caution, it may lead to negative interactions too.
Distract - postpone the urge for later. Divert attention from the urge to self-harm with escapist type behaviors to delay the urge, rather than feeling it must be confronted immediately. “I just don't want to deal with a band-aid right now so will draw a picture or go for a walk or call a friend” - sometimes pausing is enough to let the urge fade.
Grounding, nature, negative ionizers. Grounding is standing barefoot in clean soil or sandy area in nature, for 15 to 20 minutes. It can calm and recenter energy with Earth’s rhythm. Images of nature can also help calm. Negative ionizing water fountains or a salt crystal lamp can help air quality and mood.
Dissociative sensory grounding. Touch: soft velvet, polished rocks, or coins in a pocket can be a personal oasis of calm in any environment. Odor: Vanilla or other calming fragrances. Vocalize: humming, repeating a positive mantra, chanting or singing may help center or release tension. Taste: a little dark chocolate, mint, or a snack. See: Look at something in fine detail. Move: sway, spin, rock; self-soothing is at least not self-harm.
Ideas for coping with an urge to self-harm; based on "Treating Self Injury, A Practical Guide," by Barent W. Walsh, Ph.D. (2006), a guide for mental health counselors or psychologists. https://www.guilford.com/books/Treating-Self-Injury/Barent-Walsh/9781462518876

Disclaimer: This information is provided for educational purposes within the guidelines of fair use. While I am a Registered Dietitian this information is not intended to provide individual health guidance. Please see a health professional for individual health care purposes.
I have EDS and was told to drink kefir daily by a physician with the disorder as well. Obviously MCAS is part of EDS. I’ve had two rounds of EBV and CFS in my life, along with migraines.
I love Kombucha, cheese, and sour foods like kimchi, sauerkraut, ACV, etc. Wonder if eating pomegranates might make sense for me.