



What are teeth?
"Teeth are not Bones" a Twitter saga about magnesium deficiency and miscommunication, or maybe about Tribalism showing its Fangs.

Teeth are similar to bone in the shared hydroxyapatite content but are more like super hard fingernails designed for chewing, biting, and for sensing density of objects. Think about it - you know you can tell the difference between real gold and gold-plated steel just by trying to bite it. Teeth are developed in the embryo from the ectoderm layer which also becomes the skin, hair, nails, brain, nerves, and glands. Teeth are a sensory organ for pressure as well as being used for chewing and biting and they may be used in self-defense or offense.
There is more to chewing than better digestion, though. Chew your food well for better cognitive health, too. The action of chewing has shown protective benefits for the health of the hippocampus, which is the part of the brain that is damaged in Alzheimer’s dementia. (Chen, et al., 2015) Maybe smoothies aren’t the smartest choice compared to crunchier nuts or veggie sticks.
“There are multiple neural circuits connecting the masticatory organs and the hippocampus. Both animal and human studies indicated that cognitive functioning is influenced by mastication. Masticatory dysfunction is associated with the hippocampal morphological impairments and the hippocampus-dependent spatial memory deficits, especially in elderly. Mastication is an effective behavior for maintaining the hippocampus-dependent cognitive performance, which deteriorates with aging.” (Chen, et al., 2015)
My dad was a very smart man, at math and mechanical engineering and other creative tasks. He really liked crunchy things, even overly crunchy things. It is not surprising to learn that chewing is good for cognition. I am sad to report to my regular readers and anyone else, that he ate his last serving of chocolate porridge on Sunday and passed away sometime early this morning. He was a good man, with quirks and flaws, but he was loving and smart. May he rest in peace. I will crunch on in his memory. I also really like crunchy things and tend to think of smoothies as being a waste of fruit. Each to their own.
This post got extremely long, and is also a 34-page document in my Dropbox. I learned a lot about teeth along the way. There is quite a bit on magnesium and prenatal and other health issues related to tooth or bone demineralization and calcium/phosphorus/magnesium/vitamin D and Parathyroid hormone metabolism. Self-care strategies for improving dental health with diet or hydroxyapatite products are included.
Teeth seem to be more like really hard fingernails or claws but are similar to bones in the crystalline hysdroxyapatite content found in both teeth and bones.
Teeth have nonliving layers and layers with living cells and interior pulp containing a nerve and blood vessel.
Teeth contain hydroxyapatite and collagen similar to bone and also have dentin and cementum layers and contain keratin protein which is similar to hair. (Duverger Beniash, Morasso 2016; glosciencepro.com) The enamel layer is the hardest material in our body, and it and the dentin are no longer living tissue, they are more like the outer part of a fingernail or strand of hair. The cementum layer has embedded cementoblasts which remain alive and can slowly add more mineralization but do not remove any like occurs in bone. The inner pulp part of the tooth is living tissue with a nerve and blood vessel.
Tooth enamel - our pearly whites are crystalline and the hardest part of our bodies.
The enamel layer of teeth is the hardest material in our bodies - when properly made. Bones and the outer layers of teeth are made from inorganic hydroxyapatite with varying amounts and type of organic protein. In the tooth enamel the hydroxyapatite is formed into a tighter crystalline layered structure that is very hard - it is the hardest material in our bodies. Diamonds are also a very hard crystalline form. Teeth are our version of diamonds or oyster grown pearls.
Tooth enamel is formed from the exterior in an embryo or during remineralization and it is demineralized from the exterior of the tooth. Dentin, cementum and bone matrix are built and lost from within the tooth or bone.
“Enamel, dentin, cementum, and bone are natural composites of both organic and inorganic components. Bone, cementum, and dentin are specialized connective tissues, while enamel has an ectodermal origin. For the specialized connective tissues (bone, cementum, and dentin), collagen type I constitutes ~90% of their organic component;1,2 noncollagenous proteins form the remaining. On the other hand, enamel has little or no collagen, and its organic matrix is made up of noncollagenous protein, which is 90% amelogenin.3
The inorganic component of these hard tissues consists of biological apatite, Ca10(PO4)6(OH)2. Enamel has more inorganic content (~90% prismatic crystals) than dentin and bone (~70%) and cementum (45%). The unit cell of biological apatite is hexagonal in shape; repetitions of the unit cells produce crystals of various sizes. In dentin, the crystals are plate like of 50 nm length, 20 nm width, and 2–5 nm thickness.4 In bone, the crystals are known to be ~2–6 nm thick, 30–50 nm wide, and 60–100 nm long.5 However, they are bigger and highly oriented in enamel than in bone and dentin, making it the hardest tissue in the body.” (Abou-Neel, et al., 2016)
The varying amounts of inorganic and organic material gives the layers of the teeth different properties. Enamel is very hard which helps resist greater force - chewing popcorn kernels. The dentin is more porous and resilient. (Abou-Neel, et al., 2016) The dentin would help cushion the interior pulp and nerve from that great force needed to chew half-popped kernels.
“Teeth are composed of enamel, pulp–dentine complex, and cementum. Dentine forms the largest portion of a tooth. It is 70% mineralized by weight, with the organic content accounting for 20% of the matrix, and the remaining 10% being water. Type I collagen is the primary component of the organic portion of dentine, accounting for >85%, with the remaining amounts being collagen types III and V. The noncollagenous part of the organic matrix is composed mainly of dentine phosphoprotein, accounting for ~50% of the noncollagenous part. The remaining inorganic matrix is composed primarily of HA.11 Several studies have suggested that collagen in enamel matrix is completely removed with all other organic components during the course of its mineralization and maturation.12–14 These studies refuted the earlier theories that proposed that a small percentage of collagen is retained after enamel maturation.15,16 A more recent study concluded that there is minimal collagen content, mostly types I and V, found in mineralized and mature enamel in comparison with dentine.17,18” (Abou-Neel, et al., 2016)
Collagen adds cushioning to the dentin layer. Fibromyalgia and autoimmune patients may be very familiar with how much it can hurt to chew hard foods when more inflamed. The same foods you had been enjoying can leave you looking for a fruit smoothie instead. Take-home point - if it hurts everywhere in the gumline when chewing, it isn’t a toothache, it is general inflammation making the entire gumline oversensitive to what had been normal amounts of pressure on the teeth. Nrf2 promoters including pomegranate, butyrate and niacin could help reduce the inflammatory signaling throughout the body and gumline.
Vitamin C would help strengthen gum tissue and reduce bleeding risk from flossing kernels out of the teeth later on.
Specialized cells form the different layers of a tooth.
Ameloblasts form the enamel layer, odontoblasts form the dentin layer and cementoblasts form the cementum layer. Osteoblasts are bone cells and form bone matrix. The ameloblasts and odontoblasts do not remain in the layers after formation leaving a non-alive exterior to a tooth. Odontoblasts can regenerate dentin from within by adding secondary and tertiary layers of dentin. Cementoblasts and osteoblasts become trapped within the tooth cementum and bone that they build and then remain there, alive, embedded. The cementoblasts can add more cementum, but regenerates mineralization slower than the osteoblast can if there had been demineralization by osteoclasts (Abou-Neel, et al., 2016) in response to vitamin A or D signaling.
“Furthermore, these hard tissues have different regenerative capacity. Unlike ameloblasts [which form the enamel layer] and odontoblasts [which form the dentin layer and] which leave no cellular bodies in their secreted products during the later stage of apposition, many cementoblasts and osteoblasts become entrapped by the formed cementum and bone they produce, becoming cementocytes and osteocytes, respectively. Although bone is a highly adaptive tissue (ie, continually undergoing remodeling), cementum has a very slow regenerative capacity7 and is not resorbed under normal conditions. Dentin and enamel develop their definitive structure during odontogensis. Dentin has the capacity to regenerate by the formation of secondary and tertiary dentin, but enamel does not have the regenerative capacity. Unlike skeletal bones, facial bones are derived from both neural crest and paraxial mesoderm and they respond differently to growth factors and mechanical stimuli.8” (Abou-Neel, et al., 2016)
The activated forms of Vitamin A and vitamin D can cause demineralization of bone tissue.
Bones have live bone cells (osteoclasts and osteoblasts) that continually can build or breakdown bone matrix in response to vitamin D (van Driel, van Leeuwen, 2023) or vitamin A signaling. (Harvard.edu)
“Until recently, vitamin A was not part of the bone formation vs. bone resorption equation. Then laboratory studies showed that retinoic acid (which the body makes from vitamin A) stimulates osteoclasts but suppresses osteoblasts. That's why even mild excesses of vitamin A appear to increase the risk of fracture. But there's more to it, since a study of men found that a deficiency of vitamin A is also linked to an increased likelihood of fracture.” (Harvard.edu, 2014)
Demineralization and remineralization:
“Demineralization is the process of removing minerals ions from HA crystals of hard tissues, for example, enamel, dentin, cementum, and bone. Restoring these mineral ions again to the HA crystals is called remineralization. Both processes occur on the tooth surface, and a substantial number of mineral ions can be lost from HA without destroying its integrity but high sensitivity to hot, cold, pressure, and pain would be expected. Lacking of the integrity of HA latticework, however, produces cavities. Demineralization is a reversible process; hence, the partially demineralized HA crystals in teeth can grow to their original size if they are exposed to oral environments that favor remineralization.64” (Abou-Neel, et al., 2016)
Oral environments that favor remineralization; and phytates in grains, beans, seeds and some types of nuts.
Remineralization would be promoted by saliva and a diet balance that is lower in sugar content and less acidic, rather than being rich in fruit juice or acidic and/or sugary beverages. (Abou-Neel, et al., 2016) Adequate protein in the diet is needed for good saliva composition. (Johansson, Ericson, 1987) Also needed is a mouth microbiome with fewer cavity promoting bacterial species, (Kote, Kote, Nagesh, 2011; Umar, et al., 2016), and an appropriate calcium to magnesium ratio within the diet. (Uwitonze, et al., 2020)
Calcium rather than phosphorus was recommended by Abou-Neel, et al., 2016 to promote remineralization. Phosphorus tends to e plentiful and even excessive in the average diet. However excess calcium or vitamin D2 or D3 can lead to hypercalcemia. (Tebben, Singh, Kumar, 2016) So taking calcium with magnesium that is well-absorbed by the individual is a need to prevent Vitamin D signaling to the bone osteoclasts to release some magnesium. Calcium is also released at the same time proportionally whether it is needed or not.
Megadoses of vitamin D or calcium can be a negative particularly for a few health conditions as it can lead to excess active vitamin D and hypercalcemia, both of which can cause many negative symptoms. (Tebben, Singh, Kumar, 2016)
“Laboratory findings other than hypercalcemia include hyperphosphatemia and suppressed serum PTH concentrations. The presence of hyperphosphatemia is a clue to the presence of hypervitaminosis D.” (Tebben, Singh, Kumar, 2016)
Magnesium deficiency negatively affects calcium and bone metabolism and can lead to osteoporosis. Impacts on bone metabolism would have indirect impact on electrolyte balance and quality of saliva.
“Indeed, nutritional factors are of particular importance to bone health and they are modifiable by providing food-based recommendations. A correct diet is particularly important in the young, before skeletal maturity is reached. While calcium and vitamin D have been the master focus of nutritional prevention of osteoporosis, several additional food constituents—such as phytoestrogens, flavonoids, vitamins A, B, C, E, folate—and minerals among which copper, zinc, selenium, iron fluoride and magnesium (Mg), are known to be important [5]. In particular, a significant association has been found between bone density and the intake of Mg, an essential micronutrient with a wide range of metabolic, structural and regulatory functions [6].” (Castiglioni, et al., 2013)
Calcium binding phytates in grains, seeds, beans and some nuts may reduce calcium availability in a vegan or vegetarian diet that has a greater amount of those foods than average. (Brouns, 2021; Schlemmer, et al., 2009)
The phytates can bind with minerals in a reaction called chelation. “Zn2+ and Fe2+, Mg2+, Ca2+, K+, Mn2+ and Cu2+” (Brouns, 2021) may be chelated by phytates. The minerals might be from within the food item, but also could bind those in the gut acting as electrolytes, or those dissolved in the intestine from other food or supplements. The chelated minerals then exit the body in the bowel movement. (Brouns, 2021; Schlemmer, et al., 2009) Phytates have some health benefits too, (Pujol, et al., 2023); total quantity in a diet balance is the issue. Phytate content in a vegan diet may be excessive and can be a cause of demineralization of tooth enamel.
Embryogenesis of teeth and Retinoic Acid excess.
Excess active Vitamin A during very early fetal development may be able to cause gene changes that lead to weak enamel formation for the rest of the individual’s life and increased risk for cavities. A condition with those symptoms called Amelogenesis imperfecta (AI) did not have a known cause until Morkmued, et al., 2017 tested their theory that excess Retinoic Acid might be causal. Confirmatory research regarding the cause of the human condition is still needed.
The results of Morkmued, et al., 2017 animal-based study supported their theory about a possible cause of AI. See Figure 7 below. Earlier stages of development of a tooth have an internal fold called the Bud Stage, which then inverts into a double layered protrusion called the Bell Stage. Enamel is added on in layers from the exterior inward. Excess Retinoic Acid at the early Bud stage can inhibit gene expression needed to form enamel. The gene change and weak enamel formation lasts throughout the person’s life in the condition Amelogenesis imperfecta. Why though was not known. Giving pregnant animals excess Retinoic acid at different stages of the pregnancy revealed reduction of the genes involved in enamelization, more so at earlier stages. It also caused reduced ossification of bone in the fetus after only two days of the Retinoic Acid. (Morkmued, et al., 2017)

Activated Vitamin A is a teratogen in pregnancy and may cause a gene change leading to weak enamel production throughout life – and increased risk for cavities no matter how well you brush your teeth.
Please don’t drink and have babies whether you are the sperm donor (it takes 74 days to grow a sperm, during which alcohol used causes DNA damage to the sperm’s genes) or ovum carrier.
Alcohol use by a pregnant woman could cause the Retinoic Acid and gene changes seen in the animal-based study by Morkmued, et al., 2017 that might be the cause of Amelogenesis imperfecta (AI). That could mean that for some people even great oral hygiene might not protect enough against the increased risk of cavities due to weak enamel. It would be due to their mother’s use of alcohol in very early pregnancy - or her use of acne or anti-aging medications that contain active retinoids. If the father drank during sperm development than DNA changes may occur causing varied problems but not physical bone deformities as is seen in Fetal Alcohol Syndrome when a pregnant person has used alcohol, and if zinc deficient too, then the teratogenic effects can be even worse.
Retinoic Acid excess also causes osteoporosis and increased fracture risk for a person because it signals osteoclasts to break down bone and for osteoblasts to stop building new bone tissue. (Harvard.edu, 2014)
Keratin protein is in both teeth and hair and is a factor in age related discoloration.
Teeth are like hair in the shared keratin content and also in age related changes in the color according to a company who sells tooth whitening products to dentists. The shiny white of teeth fades with aging in teeth and hair loses its color as we age. They suggest that may be a visible indicator of change occurring - is your hair whiter? Then take better care of your tooth enamel too. (glosciencepro.com) ←unaffiliated
Active Vitamin A has regulatory effects on keratin production. Keratins are a group of similar proteins and are found in skin, hair, (Törmä, 2011), and tooth enamel. Keratin is used within the enamel layer of the tooth to add structural support to tightly packed rod-shaped crystals of hydroxyapatite (HA). The keratin forms a thin surface sheath surrounding each rod of HA and it seems to protect against demineralization. The rods are tightly packed together aligned vertically within the tooth rather than horizontally like in a brick wall. (Duverger Beniash, Morasso 2016)
This arrangement within tooth enamel likely increases the pressure the teeth can withstand. Picture a giant force pressing down on a stacked pile of bricks - the bricks would likely tend to fall out sideways like in a game of Jenga. If the pressure is being exerted downward on tightly packed group of four-foot-tall sections of tree trunk, arranged vertically, it likely could take a lot more force than the pile of horizontal bricks. The keratin is holding them together, though, like the mortar between bricks in a brick wall.
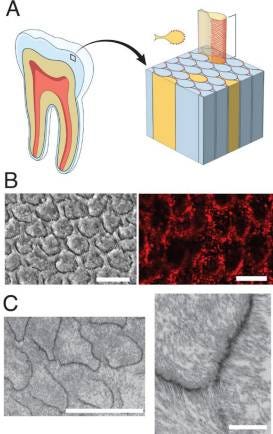
“Figure 1 Enamel structure and the presence of hair keratins in enamel rod sheaths,” (Duverger Beniash, Morasso 2016) A) shows a side view drawing; B) shows a top down view of a healthy tooth - the keratin is the darker areas surrounding hydroxyapatite crystal rods; C) shows a tooth that has lost hydroxyapatite and some keratin is still present. The keratin forms semicircles around the crystals rather than completely surrounding each rod.
Increased acidity from diet or body fluids causes hydroxyapatite crystals to dissolve.
Acidic conditions in the mouth can cause the hydroxyapatite to dissolve but it will not affect the keratin which is more resistant to acid. Drinking strongly acidic beverages regularly, like soda, lemonade, orange juice and coffee, will likely increase hydroxyapatite from tooth enamel, leading to premature aging of the teeth.
Aging causes changes in the ratio of carbonate to calcium within hydroxyapatite (HA) which can have variations rather than being pure HA. Unlike bone tissue, teeth do not have much magnesium content as it suppresses more enamel formation rather than promoting it. Less calcium and more carbonate in the mineral composition of teeth promotes dissolution of the apatite from the hydroxyapatite. Calcium loss precedes phosphorus and therefore calcium is recommended for promoting remineralization of teeth rather than phosphorus. (Abou-Neel, et al., 2016)
“With age, the crystallinity of dental HA decreased but the carbonate content increased. […] A decrease in crystallinity and increase in carbonate content favor the dissolution of dental apatite. This is a change in material phase and the composition of dental mineral, while also reducing crystal size.61 The carbonate content has a significant effect on the reactivity and solubility of physiological HA.” […]
“During demineralization, calcium release precedes phosphate release from enamel, dentin, and cementum. Therefore, using calcium rather than phosphate to suppress the demineralization process would be effective.63” (Abou-Neel, et al., 2016)
More acidic beverages or overall more acidic body fluids and saliva would increase the rate of demineralization - dissolving of the hydroxyapatite. Taking only calcium supplements without magnesium adequacy would be promoting a more acidic body pool. Tooth care needs to keep in mind that teeth are part of the body as a whole and that taking only calcium will not necessarily provide calcium to the teeth. If high dose calcium supplements are shifting the body towards acidity, then it could increase loss of tooth enamel instead of helping.
Magnesium deficiency and calcium excess is common in the US and adds to demineralization of tooth enamel which then is more cavity prone.
Magnesium deficiency in pregnancy can be a factor in both osteoporosis risk and dental problems but not for the same reasons. The mechanism of action is different. Demineralization of enamel occurs in a higher calcium or increased acidity level and reduced saliva can also increase risk. It is a chemical process occurring based on the fluid bathing the mouth and teeth from saliva or food or beverages. Osteoclast bone cells are directly removing calcium and magnesium from bone in response to signaling by activated forms of vitamin A or D.
When there is an increased ratio of calcium to magnesium it can cause bone loss and also increase tooth demineralization which increases risk for cavities. (Uwitonze, et al., 2020) Prenatal patients and everyone else too, roughly in the US, are told to take a lot of calcium supplements and rarely any magnesium. If magnesium is recommended, a lower amount is recommended compared to our need for it than for calcium. Calcium recommendations in the US tend to be for a good bit more than we need and magnesium recommendations are for slightly less than we probably need.
Excess calcium in ratio to magnesium can cause softer enamel that is more cavity prone. (Uwitonze, et al., 2020)
“Taking calcium without magnesium results in soft dental enamel, which cannot resist the acids causing tooth decay.” (Uwitonze, et al., 2020)
Magnesium deficiency also causes insulin resistance, and higher blood sugar causes more sugar in the saliva, adding to cavity risk.
Magnesium deficiency causes insulin resistance, (Milagros, et al., 2005; Nadler, et al., 1993) , hyperinsulinemia, and high blood pressure. Increased sugar concentration in blood plasma also means there will be increased sugar concentration in the saliva - increasing cavity risk. Insulin resistance is a risk factor for periodontal disease. Worse insulin resistance was associated with more severe periodontitis, even when weight was within the normal range of BMI. (Sun Oaks Dental)
“We conclude that dietary-induced magnesium deficiency 1) increases thromboxane urinary concentration and 2) enhances angiotensin-induced aldosterone synthesis. These effects are associated with a decrease in insulin action, suggesting that magnesium deficiency may be a common factor associated with insulin resistance and vascular disease.” (Nadler, et al., 1993)
Protein and saliva, and age-related changes in need for dietary protein.
A low protein diet might affect health of the mucous membranes and muscles of the mouth in addition to reducing immune function and saliva. Our body fluids need albumin protein to help maintain function. When we age, we need more protein in our meals throughout the day as the body doesn’t store it as well and will take protein from body parts, muscle primarily, to use for essential functions or for energy if intake is too low in calories also. Albumin levels in blood plasma would drop also and edema might occur.
On average females have a reduced salivary flow compared to males and elderly people have reduced flow compared to younger people. Less saliva is linked to more risk for cavities or other dental conditions. During inflammatory conditions including gingivitis and periodontal disease, albumin levels can rise in addition to other proteins, and was found to be significantly elevated in saliva which can be used as a lab test biomarker for illness. Salivary albumin levels were doubled in gingivitis and quadrupled in periodontal disease. (See Table 1, Shaila, Pai, Shetty, 2013)
Senior Citizens can help prevent age-related muscle loss (and maybe help preserve saliva and tooth enamel) by aiming for 20-30 grams of protein at breakfast, lunch, and dinner, instead of having a standard US high carbohydrate breakfast and a big meat entree at dinner. DHEA taken as a supplement starting at age 35 may also help preserve muscle: 25 mg for females, 75 mg for males. (Search term to look for more info - ‘sarcopenia’.)
Female hormones or immune signaling modify saliva during pregnancy making it less antimicrobial.
More sugar or acid in the saliva and a higher ratio of calcium to magnesium can all lead to more demineralization of tooth enamel and more cavity promoting bacteria. During pregnancy, increased estrogen levels [*or immune signaling] modify a woman’s saliva in a way that makes it lower in volume and to have less antimicrobial power against cavity promoting bacterial species. Anthropologists found that female skeletons on average had more tooth decay than male skeletons on average. (Xiao Dental)
“Women naturally produce less saliva than men, reducing the removal of food residue from teeth and promoting dry mouth. During pregnancy, the chemical composition of saliva changes, reducing saliva's antimicrobial capacity.” (Xiao Dental)
TRP channel activators may stimulate more saliva production such as capsaicin in hot pepper and mint, but cinnamon was not found to have much effect.
“Major salivary glands and minor salivary glands beneath the oral epithelium secrete saliva in response to chemosensory stimulation of trigeminal nerve endings by capsaicin, nonivamide and other TRPV1 agonists.97 Menthol, a TRPM8 agonist, can also increase saliva secretion and modulate the protein composition of saliva, but cinnamaldehyde, a TRPA1 agonist, had relatively little effect on salivation.97” (Houghton, et al., 2020 cited by Arendt-Nielsen, et al., 2022)
From reference 97: black pepper/piperine is another TRP activator that can increase saliva. Protein content in saliva can be effected by chewing and delicious odors can also increase saliva. (Houghton, et al., 2020)
“Specific protein changes in saliva in response to differing stimuli are possible because of the many sources of proteins which are likely to respond differently to different nerve mediated stimuli. For example, the submandibular and sublingual glands secrete in response to olfaction (37) whereas the parotid glands do not (38). Conversely, the parotid glands are preferentially stimulated by chewing which results in a higher amylase output (39). In these scenarios, proteins associated with specific glands, e.g. higher amylase secretion by the parotid glands or mucin secretion by the submandibular and sublingual glands, will have a relatively increased abundance when compared with unstimulated levels.” [97]-(Houghton, et al., 2020)
Pomegranate products for a healthy mouth microbiome.
The simple solution for an unhealthy microbiome in the mouth is to drink one ounce of pomegranate juice daily (Kote, Kote, Nagesh, 2011) or use pomegranate peel extract/strong tea as a mouth-rinse daily. (Umar, et al., 2016) The pomegranate is a strong enough antimicrobial agent that it reduces cavity promoting species in the mouth like S. mutans. Pomegranate products are also anti-inflammatory, wound healing, and promote beneficial microbiome species in the gut too. The extract study by Umar, et al., also observed an increase in the pH level of the mouth, more alkaline, less cavity promoting, at ten minutes after the mouth-rinse was used (measurements were taken at three time-intervals, ten minutes was the first interval). (Umar, et al., 2016)
Hydroxyapatite - commercially available remineralization product - bioidentical, safe enough for children.
Hydroxyapatite as a topical application or in toothpaste, has been found to help remineralize thinning enamel in children’s teeth and is safe as it is bioidentical to the pure form we might make for ourselves (pure ~ no carbonate swap or other minerals besides calcium). (Meyer, et al., 2022)
"Biomimetic hydroxyapatite [HAP; Ca5(PO4)3(OH)] is known to have favorable remineralizing properties combined with an excellent biocompatibility, i.e., it is safe if accidently swallowed." (Meyer, et al., 2022)
Hydroxyapatite is recommended by a dentist as helpful and safe for pregnant women, children and people who may be at risk for fluorosis. (johnrstriebeldds.com) It likely would also help people on a vegetarian or vegan/no animal products diet at risk from phytates.
“Hydroxyapatite is biocompatible and non-toxic as it is a naturally occurring mineral found within our bodies. There is no risk of overexposure as there can be when using fluoride-based products. It is ideal for children, pregnant women, and those at high risk of developing fluorosis.” - John R. Striebel, DDS, (johnrstriebeldds.com)
Toothpaste with hydroxyapatite (HAP in this article) has been found effective for cavity remineralization and reducing tooth sensitivity. The dissolved hydroxyapatite will join the crystalline lattice of the tooth enamel hydroxyappatite. Otherwise remineralization would occur only in the presence of enough calcium and phosphate that it precipitates onto the tooth enamel as calcium phosphate. (O’Hagan-Wong, et al., 2022)
“Under normal conditions, there is a dynamic balance between HAP mineral in the tooth structure and in the oral fluids [9]. Demineralization refers to the net loss of calcium and phosphate ions from the tooth structure whereas remineralization is the addition of calcium and phosphate back into the enamel structure from supersaturated oral fluids (i.e., precipitation of calcium phosphate).” (O’Hagan-Wong, et al., 2022)
Braces - new biotech that left some damaged teeth and jaws.
The pressure of metal braces for straightening teeth on the jawbone cause osteoclasts in the jaw to breakdown bone at the pressure points and for osteoblasts to rebuild the jawbone away from the pressure points, which allows the teeth to gradually take on new positions within the gumline. (caortho.org) Cautionary note - it turns out that some children/teens who had to wear braces ended up with permanent problems with their teeth or jawbone. See: Risks of Dental Braces, (news-medical.net); or more extensive: Complications with Braces, (Thangamani, 2017).
New biotech is not always safe biotech.
Take-home tips from above and mentioned later -
Hydroxyapatite toothpaste or topical products for remineralization.
Pomegranate products for improving microbiome species in the mouth and gut.
Adequate protein food to promote good saliva flow and composition - but not a high protein diet if pregnant (greater than 20% of total calories possibly, Carnivore diet could be a risk to the fetus. Higher protein intake can be a danger to the developing baby as the waste products can affect methylation cycles negatively and lead to excess homocysteine and ammonia production. The ammonia is dangerous to the fetus - deadly even. (Herring, et al., 2018)
Adequate magnesium in proportion to total calcium from diet and supplements, Excess calcium/magnesium ratio may demineralize enamel. Magnesium deficiency can cause insulin resistance and hyperinsulinemia and that can increase periodontal disease. Magnesium deficiency also reduces immune function adding to mouth microbiome risks.
Adequate sunshine and/or vitamin D3. The immune system of a pregnant woman is suppressed to protect herself and the baby from autoimmune reactions against the other’s not-exactly-matching DNA. This immune suppression is seen in saliva too and increased risk of cavities can occur. Vitamin D has control over the tolerance promoting Treg regulatory T cells. (Moldenhauer, et al., 2022) Adequate magnesium and protein are also a need for vitamin D metabolism to function and zinc is needed for thymus gland function and Treg cell formation. Avoiding glyphosate is likely a need as it may be inhibiting normal vitamin D metabolism, which would make vitamin D3 supplements the more bioavailable form over the more common D2 supplements.
Avoid excess sugar and carbohydrates as it increases risk of high blood sugar and insulin resistance, (which can also negatively impact vitamin D and Treg cells), *but also avoid a high protein diet (above 20% of total calories) if pregnant. (Herring, et al., 2018)
Acidic beverages or a more acidic/inflamed body can increase demineralization as the hydroxyapatite is dissolved in more acid solutions.
Leg cramps that don’t respond to magnesium and/or potassium foods, Epsom salt soaks, or supplements, may be a symptom of over-acidity. Having a sudden urge to urinate and then only producing a tiny bit which ay sting or burn a little is also a sign of the body trying to get rid of excess acidity. Any inflammatory condition is likely to include more acidity than in normal health. Taking very small amounts of baking soda in water, drink to taste, may help with leg cramps that aren’t being helped by magnesium and potassium.
Teeth and Tribalism
I made the mistake of making a negative comment about a dentist who seems to have sensitive feelings and also a large posse of tribal members who reacted en masse on Twitter. Just a fun game of winner/loser it seemed - the prenatal patients of the dentist not willing to accept new information being the losers in this game. I apologized and shared links supporting my concern about magnesium deficiency in pregnancy.
My initial reply was about magnesium deficiency being common in pregnancy and a likely factor in tooth decay during pregnancy instead of “subpar hygiene” by any pregnant woman with tooth problems during their pregnancy. That reply got a non-response about the magnesium issue by the anonymous dentist and instead he/she/they focused on my error in saying “teeth are bone”….that can demineralize similarly to bones - is what I meant - and which I was wrong about the details. Demineralization occurs from teeth due to acidity not because of hormonal signaling to osteoclasts in bone.
“Teeth are not bones” and are no longer mainly classified as part of the skeletal system.
It turns out that the medical industry has now classified teeth as part of the digestive system and in a few places, teeth are still mentioned as being part of the skeletal system. Teeth have connections with both systems would be the simple way to look at that. And they are present in a skeleton after the stomach, gums, and rest of the digestive system have decomposed - so any grade-schooler is going to think teeth do go with skeletons. That is about labeling, industry jargon, more than a definitive line in the sand declaring that teeth are only part of the digestive system.
“Teeth are considered part of the skeleton system even though they are not bone. Teeth are the strongest substance in your body being made up of enamel and dentin. There are 32 teeth in an adult, and 28 in children.” (Kim/Skeleton)
“Teeth are not bones,” is kind of an inane statement in that it doesn’t say what teeth are; it just states what they are not. Are teeth like stomach tissue? No.
It turns out that the search results are full of that approach to defining teeth, the anonymous Twitter dentist is not alone in focusing on that phrase - teeth are not bones. The search flipped “What are teeth?” to variations of “What are teeth made of?” or the popular “Teeth are not bones”. Well then, what are they?
If a visiting alien asks, “What are teeth?”, answering with “Teeth are not bones”, doesn’t help at all. Alien: “What are bones?” This is like the “Defining a word with the word” error. You can’t define a word with the same word or with only a negative of what it is not. A negative is just one step on the Differential Diagnostic tree of ruling out knowns from an unknown. ‘This’ is not ‘that’ - okay, so what is ‘this’?
The Glo Science Professional tooth whitening product got closest to my embryology-based answer with their comparison of keratin in hair and tooth enamel and age related discoloration. (glosciencepro.com)
The main replies with substantive value (rather than nasty comments about my appearance or intellect or need for tooth whitening strips) stated that teeth are different than bones because they don’t have osteoclasts and osteoblasts which can demineralize or remineralize the bone matrix from within the bone. I was told that teeth also don’t have collagen like bones have which I have since learned was wrong. A reply that I said was wrong at the time was based on a Healthline article, stating that teeth have “no living tissue”. That simply seems false or another odd jargon thing.
There is an inner pulp area at the interior of the base of teeth that is living tissue and the cementum layer does have a few living cementocytes that can slowly remineralize tissue but do not generally resorb it like osteoclasts resorb calcium and magnesium from bone tissue. Dentin may be able to be replenished by odontoblasts with addditional layers being added from within the tooth. The odontoblasts must remain in the pulp area as they do not become embedded like the cementoblasts. (Abou-Neel, et al., 2016)
What are teeth then? - answer - part of my job as a dietitian since they are considered to be part of the digestive system.
What I learned on my own about teeth, after thinking about differences such as the fact that we only have one set of bones for our lifetime, but we get baby and adult teeth, is that teeth must be more like specialized fingernails or rounded claws. (Morkmued, et al., 2017) But are located within the gumline and partially embedded within the jawbone. If the tooth-fingernails were more like a cylinder shape with a live nerve and blood vessel tucked in the very middle layer of pulp towards the base and roots of the tooth - then it makes sense - like an arcing cylindrical cat claw or snake fang.
Hardened enamel is the very outer layer of a tooth and it is crystalline - smooth, shiny and hard. Softer (but still hard) mineral based dentin and cementum layers form the interior part of the tooth. The outer enamel and dentin layers are not ‘alive’ - that is the fingernail or claw part of the tooth and there is a smaller pulp center that does have a living nerve and blood vessel with some mineralized matrix. Picture a pet’s claw that you can’t clip too short, or it hurts them.
Teeth might fit better within the skin and sensory systems as they contain nerves and are derived from the same ectoderm layer of the embryo. Think of how sensitive teeth are when there is dental pain, or more pleasant, the crisp crust on fresh baked bread. A cat can tear into flesh or delicately warn a human to stop petting now. A mother cat can gently carry a kitten with her teeth, or bite to kill when catching a mouse.

What are teeth? Teeth are like bony fingernails used for chewing or catching food. The enamel is derived from the ectoderm layer during embryogenesis which also will form our skin, hair, finger- and toenails, and our brain, nerves and endocrine glands and the cornea and lens of the eyes. The dentin and cementum layers of teeth are derived from connective tissue which is formed from the mesoderm layer along with bone and muscle (cardiac, skeletal and smooth muscle tissue).
While teeth are sometimes classified as part of the skeletal system, they are now considered part of the digestive system as we chew with them and more mastication aids in digestion. The gastrointestinal tract includes cells from all three embryotic layers. “The gastrointestinal (GI) system involves three germinal layers: mesoderm, endoderm, ectoderm.” (CC BY-NC-ND 4.0, Bhatia, Shatanof, Bordoni, 2023)
Teeth are hard crystalline pressure sensitive sensory organs embedded within the jawbone and are made up of compounds similar to bone - hydroxyapatite, and hair -keratin, and unique to teeth - also layers of dentin and cementum. The hard outer layers are not alive but protect an interior pulp layer that has a nerve and blood vessel.
Teeth are used for gauging hardness of substances, doneness of cooked food, and are used for chewing food which aids digestion, or for tearing or cutting small items. Teeth can also be used defensively or offensively in a warning snarl or bite.
The BowTied Gator dentist couldn’t let this go - two women disagreeing with his Tweet. I did call it the stupidest I had read and I still consider “Teeth are not bones” as only being half of a complete sentence - “Teeth are not bones, they are…”.
He stated in a long Twitter post, copied below and fact checks added by me, that he is protecting pregnant women from disinformation about magnesium and protein having a very large role in oral health. The risk being that a pregnant woman might take a magnesium supplement and a protein bar and feel safe regarding oral health . . . and maybe not brush their teeth. Implied suggestion again that women are just bad at tooth-hygiene. Yet he didn’t really show that he understands magnesium’s role in dental health or prenatal care or heard what I was trying to say; or understands the role of protein adequacy in saliva quality. And he cited a 1969 and a 1975 paper as references for trivial things like immune function during pregnancy and calcium metabolism.
Immunology has had a hard time during CoV era, but it has come a long way since 1969. Calcium metabolism research papers seems to have stalled out in the US as being only about calcium, vit. D, PTH, and phosphorus, and frequently has NO mention of magnesium. I find more informative reviews and research by people in other nations. Seriously odd when papers on topics that involve magnesium include zero mentions of the word.
He has a lot of BowTied buddies though and is getting a lot of views of his takedown about “Teeth are not bones.”
Then what are teeth? He doesn’t really tell us that.
There was a swarm of “BowTied____” accounts who mostly had nasty things to say about my appearance, eyes or teeth, or intellect, or mental health, and also tried to silence the other woman and call her a Loser. Were they a football fan club I wondered? Why be so combative over dental care during pregnancy? Florida Gator fans?
No, search results suggest they may be part of an online group that may be loosely organized around cryptocurrency and have a focus on business building by supporting each other’s business efforts even though they are anonymous and you wouldn’t know how good their work was - kind of like the insider cult working together exclusively whether very talented or not. Unless it was an anoymous online business with a customer review area. My mentioning cryptocurrency got some pushback, suggesting not all BowTied anons use crypto. (ref1) They did all seem to be good at “Tuesday Trolling” (ref2) All work and no play, you know, makes Jack a dull boy. Again, the prenatal patients of the dentist are the losers here.
The dentist and crew also consistently called me a nutritionist or ‘meme nutritionist’ instead of using my credentials, Registered Dietitian. Ancillary Health Professionals ideally communicate with each other and respect each other’s specialties. Anyone who isn’t named Dunning-Kruger knows that it is impossible to be aware of all areas of research and medical science or individual health variations.
Grab some popcorn, we will be fact checking the fact checker. I left the typos alone.
@ BowTiedGatorDDS’s “Teeth are not Bones” takedown of me and another female Tweeter, 10:13 AM · Jul 16, 2023:
“Are teeth bones? According to resident nutrionist @deNutrients it is a resounding yes. Does lack of protein cause cavities during pregnancy? According to our resident Art and Literature expert, @meghaverma_art the answer is "Absolutely" This is going to be a long post, not because I want to but because it is my responsibility. I'm up early on a Sunday typing a rebuttal to two midwits who feel the need to comment on something that is not within their domain. Why? I have no idea, but as a self-proclaimed educational vigilante, we must protect and serve.
ARE TEETH BONES? Simply, no they are not. But let's get into the details.
Composition: Both teeth and bones are hard, white, and contain calcium, but that's where the similarity ends. The majority of a tooth is made of dentin, which is calcified connective tissue that provides the tooth with its basic shape and rigidity. The outermost layer of the tooth is the enamel, which is the hardest and most mineralized substance in the human body. It's composed of approximately 96% mineral (mostly hydroxyapatite), 3% water, and 1% organic material. In contrast, bones are composed of about 50% mineral (also largely hydroxyapatite), 25% water, and 25% organic material, including collagen. This composition gives bones strength and flexibility.

Function: Bones serve many functions including supporting the body, protecting organs, producing blood cells, and storing essential minerals. Teeth, on the other hand, are mainly for biting, cutting, and grinding food.
Regeneration: Bones have the ability to regenerate and heal themselves if fractured. They are constantly undergoing a process of remodeling, where old bone is resorbed and new bone is formed. Teeth cannot regenerate in the same way. Once tooth enamel is lost, it does not regrow, and cavities cannot heal themselves. Dentin can be regenerated to a very small degree, but it happens from within the tooth not from without.

Blood Supply: Bones contain bone marrow. Teeth, on the other hand, have a pulp which contains a blood vesel, and nerve. The types of tissue are completely different and have almost nothing in common. Now that we've discussed the differences between teeth and bones, we can pick apart her argument that the child creates a demand for calcium due to low magnesium.”
[*That was not my argument at all - low magnesium intake for a pregnant person, or anyone, causes a demand for magnesium release from the bones, where about half of the body’s stores of magnesium are located (~50%). Magnesium is then removed from the bones along with calcium whether more calcium is needed or not, due to vitamin D signaling. The body needs magnesium and it will do a lot to maintain magnesium levels within the blood (1% of total) and cells (~ 50% of the total body store of magnesium), (Cappadone, et al., 2021), including taking it from the bone storage. And that leads to osteoporosis risk; the demineralization of enamel with magnesium deficiency is for other reasons related to the excess calcium/too little magnesium ratio. (Uwitonze, et al., 2020)
Pregnancy doubles the need for magnesium according to a review on bone health: “During the childbearing period, pregnancy, and breastfeeding, the demand for Mg doubles. This is due to the needs of the growing fetus, the placenta, and the increase in the body weight of the pregnant woman [62].” (Ciosek, et al., 2021)
“Magnesium deficiency has an impact on bones by affecting the main regulators of Ca homeostasis―PTH and 1,25(OH)2 D3. Hypomagnesaemia prevents the release of PTH and possibly also reduces sensitivity to circulating PTH in target organs, thus producing a biochemical pattern identical with primary hypoparathyroidism [70]. Supplementation of Mg has been shown to correct the levels of PTH and 1,25(OH)2 D3 in osteoporotic postmenopausal women [71]. Moreover, the level of 1,25(OH)2 D3 in diabetic patients with low Mg levels returns to normal after Mg supplementation [72].” (Ciosek, et al., 2021)]
“Don't get me wrong, I'm a huge proponent of taking magnesium. I take it daily. While magnesium is a crucial mineral for overall health, including bone and tooth health, a direct connection between low magnesium levels and tooth decay is not evident. Instead we have a myriad of other strongly understood mechanisms in which pregnant women take a sharp turn for the worse with regard to oral health. Ah, what a relief. Now we can move on from the boring topic of "teeth are bones". Next up we have this ice cold take:

She uses vegans as proof that protein is why saliva quality is the only reason for pregnancy cavities. Low protein during pregnancy is a huge problem, and leads to serious effects on the mother and baby, but cavities are not one of them. [Herring, et al., 2018] https://ncbi.nlm.nih.gov/pmc/articles/PMC5882021/ It is possible after reading that link, that @meghaverma_art mother did not have adequate protein intake during pregnancy. These two takes are not "WRONG WRONG WRONG" They are instead, half true. Which is more dangerous, because pregnant women may see this and say "wow all I need is a quest bar and a magnesium pill and I'll be cavity free! No, you won't.”
[Low or high protein intake in pregnancy causes severe consequences to the fetus, but his citation has nothing to do with dental health in pregnant women. It has to do with arginine and methylation cycle dysfunction on a higher protein diet (>20% of Total calories. A carnivore style diet would be dangerous and might lead to miscarriage or neurocognitive problems in the fetus. (Herring, et al., 2018)
This link I found does have to do with dental health and a low protein diet in animals: “We tested the hypothesis that a low protein diet (5%) would change the conditions for synthesis and release of protein from the salivary secretory cells and increase caries development. … After an experimental period of nine weeks the animals fed the 5% protein diet had lower body weights, saliva secretion rates and total protein secreted per minute than a control group fed a 20% protein diet. There were greater numbers of cariogenic streptococci on the teeth and the caries scores were higher in the rats fed the low protein diet than in the rats in the control group.” (Johansson, Ericson, 1987)
A pregnant woman who has hyperemesis for the first trimester may only be eating potato chips and lemonade on most days which would be a 0.0 % protein diet, but it can also be easy to get too little protein in a diet focused on carbohydrates, or it may be expensive to get enough protein foods on a limited budget.
Changes in saliva flow and composition were found in a simulation of Kwashiorkor, a protein malnutrition, in an animal-based study. “These findings suggest the role of functional and biochemical changes in salivary secretion in the pathophysiology of oral diseases associated with protein malnutrition.” (Lasisi, Alada, 2015)
I’m with Megha on this one and when did she mention vegans in the screenshot above?]
“Here's what @deNutrients and @meghaverma_art should have said, but didn't because they don't know what they are talking about:
PREGNANCY AND TEETH During pregnancy, a woman's body goes through a myriad of systemic changes. Some of these changes can contribute to dental issues, including cavities. Let's explore these in detail:
Hormonal/Microbiome Changes Pregnancy triggers fluctuations in hormone levels, (increases in progesterone and estrogen.) This hormonal shift leads to "pregnancy gingivitis," an inflammation of the gums that can cause swelling, tenderness, and bleeding. This allows the proliferation of anaeobic bacteria which cause cavities and gum disease. [Wu, Chen, Jiang, 2015] https://ncbi.nlm.nih.gov/pmc/articles/PMC4385665/”
[The review article concludes that it is not known why there is a correlation between pregnancy hormones and gingival inflammation:
“Based on the data described above, the connection between increased plasma levels of pregnancy hormones and a decline in periodontal health status exists. In addition, the influence of sex hormones can be minimized with good plaque control. From above, it can be assumed that the fluctuation in estrogen and progesterone levels during pregnancy exerts the influence of subgingival microbiota and a spectrum of inflammatory responses in gingival tissues through the changes of chemotaxis, cytokines, enzymes, and antioxidants from PMNs, GFs, and PDLCs and thus indirectly contributes to increased gingival inflammation. The mechanisms responsible for these changes are not fully known.” (Wu, Chen, Jiang, 2015)
They could read this for some enlightenment: (Moldenhauer, et al., 2022), discussed shortly later.]
“Changes in Diet and Eating Habits Many pregnant women have cravings, which usually leads to an increased intake of process carbs/sugars, fuel for cavity causing bacteria. Acid reflux or morning sickness can also expose teeth to stomach acid, which can erode enamel and make teeth more susceptible to cavities.”
[Partially true - pregnant women can have increased cravings but it may be for potato chips and lemonade, not always for sweets or for the stereotypical claim of pickles and ice cream. Hyperemesis (morning sickness) would be a tooth decay risk due to the acidity.]
“Decreased Immune Response Pregnancy is a state of immune modulation, where the body balances between protecting itself and not rejecting the baby. This can lead to a decreased immune response in the gums, making them more susceptible to bacterial accumulation and potentially to cavities. [Hartzer, 1969] https://ecommons.luc.edu/cgi/viewcontent.cgi?article=3367&context=luc_theses”
[This is an ancient study, but interesting background finding regarding changes seen in the gingiva during pregnancy: “A more recent study involving the attached gingiva in pregnancy by Turesky, Fisher, and Glickman (1958) has shown a relative increase in epithelial glycogen, reduction in glycogen and carbohydrate-protein complexes of the connective tissue, and a thinning of the basement membrane.” (Hartzer, 1969)
The experiment in the thesis paper used Radioactive iodine labeled antibodies for cavity promoting bacterial species to 19 pregnant women and a control group of 19 non-pregnant women. The women’s saliva was sampled in order to measure the antibody response for the cavity promoting species. The immune response of the pregnant women seemed reduced compared to that of non-pregnant women. Pregnant women with inflamed gingiva had a greater response than the pregnant women without inflamed gums. (Hartzer, 1969) And their developing babies all got a dose of Radioactive iodine.
Newer research has filled in a lot since 1969. That was an amusing read/trip back in time except for the pregnant women getting radioactive iodine. Vitamin D is so critically important and found in greater amounts in the placenta than other organs because it promotes regulatory T cells (Treg). To accept the foreign DNA of the baby the mother’s immune reactivity throughout the body is tamped down and the increase in Treg Tcells help prevent autoimmune antibody formation. This does leave pregnant women at more risk for catching a cold or other infection and the traditional approach was for her to avoid big public events. Reduce stress, take it easy is healthy for mom and baby.
“Pregnancy depends on a state of maternal immune tolerance mediated by CD4+ regulatory T (Treg) cells. Uterine Treg cells release anti-inflammatory factors, inhibit effector immunity, and support adaptation of the uterine vasculature to facilitate placental development. […] We describe how hyperglycemia and insulin resistance affect T cell responses to suppress generation of Treg cells, summarize data that implicate a role for altered glucose metabolism in impaired maternal-fetal tolerance…” (Moldenhauer, et al., 2022)
Magnesium deficiency could cause insulin resistance and negatively impact vitamin D metabolism and Treg cell production leaving the pregnant person at risk of autoimmune disease antibodies forming against the baby’s DNA or other foreign dietary proteins - and increase risk of periodontitis. (Sun Oaks Dental)
Magnesium deficiency also causes inflammatory signaling (Ciosek, et al., 2021) which would be a negative for dental health or overall health.
“As recent studies show, Mg deficiency triggers an inflammatory response, which results in the activation of leukocytes and macrophages, the release of inflammatory cytokines and acute-phase proteins, and excessive free radical production [73,74]. The inflammatory response mechanisms in Mg deficiency probably include: 1) the influx of Ca into cells and the priming of phagocytic cells; 2) the opening of Ca channels and the activation of NMDA receptors; 3) the release of neurotransmitters, such as substance P; and 4) the oxidation of the membrane and activation of the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) [75]. Released proinflammatory cytokines play a potentially critical role in both the normal process of bone remodeling and in the pathogenesis of perimenopausal and late-life osteoporosis [76].” (Ciosek, et al., 2021)
Balance is critical with magnesium and calcium or phosphorus and calcium according to the review on bone health by Ciosek, et al.. Too much magnesium in ratio to calcium is also bad for bone health. Calcium and phosphorus may be best in a 1 to 1 ratio for bone health however there is more of a tendency for excess phosphorus and low calcium in many people’s diets (or beverage choices). Low calcium with a high intake of phosphorus is a risk for osteoporosis possibly because of secondary hyperparathyroidism and increased phosphorus may inhibit osteoclast differentiation and activity. Low calcium was approximately 400 mg/day in one study “[104]” cited by Ciosek, et al., 2021.]
“Changes in Oral Care Routine Some pregnant women experience an increased gag reflex, leading to difficulties in maintaining their regular oral hygiene practices. This, along with possible changes in sleep patterns, physical discomfort, and fatigue, can sometimes lead to less optimal oral hygiene during pregnancy. How do I know this? Not because of my degree in art, but rather the thousands of pregnant women I've seen as patients. [Arima, et al., 2022] https://pubmed.ncbi.nlm.nih.gov/36163018/”
[Good to know: The study by Arima, et al., found more frequent tooth brushing and more frequent replacement of the toothbrush improved ratios of negative dental bacterial species and may reduce risk of preterm and/or Low Birth Weight deliveries - in Rwanda. (Arima, et al., 2022)]
“Changes in Saliva Composition Some research suggests that pregnancy can affect saliva's quality, altering its mineral composition and buffering capacity. This can potentially impact the natural protective functions of saliva and contribute to an increased risk of tooth decay. [Yousefi, Parvaie, Riahi, 2020] https://pubmed.ncbi.nlm.nih.gov/32718487/”
[“The results showed that salivary calcium concentration decreased in the third trimester, salivary phosphate decreased in the second and third trimesters, saliva hydrogen ion concentration decreased in the first and third trimesters, stimulated saliva flow rate increased in the third trimester, and salivary S mutans count increased in the second and third trimesters. In addition, the results showed that saliva calcium, phosphate, S mutans, and buffer capacity amounts had changed from the first trimester to the third.” (Yousefi, Parvaie, Riahi, 2020) *They didn’t assess any magnesium levels, either plasma or intracellular red blood cell.]
“Calcium Metabolism Changes There's a common belief that the baby draws calcium from the mother's teeth if dietary calcium is inadequate, but this is a myth as demonstrated by the weird pushback on my tweet yesterday. The calcium for the fetus is drawn from the mother's bones if dietary intake is insufficient not the teeth. [Pitkin, 1975, *discussed below] https://pubmed.ncbi.nlm.nih.gov/1090175/ So there you have it. Taking care of your teeth during pregnancy is an uphill battle, but it's completely possible. I manage 4-5 pregnant women at any given time, and I have methods to get them to a place of stability and adequate oral health. Optimal oral health is never the goal because pregnant women have bigger priorities than their teeth. My goal is to just maintain them until the body has a hormonal balance again.” @ BowTiedGatorDDS
10:13 AM · Jul 16, 2023 · 87.3K Views
Interestingly, magnesium is dismissed as important but having no evidence of a role in prenatal dental health. BowTied Gator DDS includes no citations supporting that claim and his citation for calcium in pregnancy opens with this clearly erroneous statement from a 1975 review paper on calcium:
“Calcium metabolism in pregnancy is a complex process involving calcium, phosphorus, vitamin D, parathyroid hormone (PTH), and calcitonin (CT) [*and magnesium]. Calcium absorption is enhanced in pregnancy, and increased storage in the maternal skeleton probably occurs as well. Adequate amounts are provided by the current Recommended Dietary Allowance of 1,200 mg.” (Pitkin, 1975)
See this more recent work for more about calcium metabolism. It is regulated by vitamin D, parathyroid hormone, and calcitonin and it affects bone health and body fluid mineral balance. But it involves other trace minerals too: iron, zinc, copper, phosphorus and magnesium. (Ciosek, et al., 2021)
“Bone is continuously remodeled by alternating resorption and accretion. The balance between these two is tightly regulated by mechanical and hormonal stimuli to keep the bone structure. An imbalance leads to pathologies, such as osteoporosis, characterized by low bone density [3]. Bone growth and metabolism are also modulated by trace elements, such as iron (Fe), zinc (Zn), copper (Cu), calcium (Ca), phosphorus (P) and magnesium (Mg). It is assumed that both deficiency and excess of the trace elements may be a risk factor for the development of bone diseases such as osteoporosis [4,5].” (Ciosek, et al., 2021)
Magnesium deficiency modifies the regulatory effects of the vitamin D and parathyroid hormone over calcium metabolism. (Ciosek, et al., 2021) So, what is playing boss in that scenario? The vitamin D and PTH or the lack of magnesium?
“Magnesium deficiency has an impact on bones by affecting the main regulators of Ca homeostasis―PTH and 1,25(OH)2 D3. Hypomagnesaemia prevents the release of PTH and possibly also reduces sensitivity to circulating PTH in target organs, thus producing a biochemical pattern identical with primary hypoparathyroidism [70]. Supplementation of Mg has been shown to correct the levels of PTH and 1,25(OH)2 D3 in osteoporotic postmenopausal women [71]. Moreover, the level of 1,25(OH)2 D3 in diabetic patients with low Mg levels returns to normal after Mg supplementation [72].” (Ciosek, et al., 2021)
A 1985 paper by the same author does mention hypomagnesemia, see quote below. Background info - when magnesium levels are low the body will try to make calcium and potassium levels lower too, in balance electrically or the excess calcium ions would be dangerous as an oxidant and can lead to overactivity and cell death when there is a lack of magnesium to block TRP channels to the extracellular calcium which is in greater concentration than within cells. Magnesium deficiency is a direct cause of insulin resistance and hyperinsulinemia and can lead to Type 2 Diabetes or Gestational Diabetes. It also is a cause of high blood pressure - hypertension.
“Diabetes in pregnancy is associated with disturbed neonatal calcium homeostasis, perhaps due to chronic hypomagnesemia.” (Pitkin, 1985)
Women can get more osteoporosis damage from a pregnancy with insufficient magnesium - because the bones release calcium along with the magnesium that the body is signaling for. Magnesium deficiency, hypomagnesemia, is frequently seen in patients with osteoporosis (30-40%, more often menopausal than younger women). (Rondanelli, et al., 2021)
Magnesium deficiency is more common than realized and the recommendations for intake may be lower than required for optimal health.
“The RDA values for men and women diverge after this age, and men normally require more Mg2+ than women, depending on their larger body mass. Furthermore, it has to be pointed out that pregnancy and lactation dictate an about 10% higher supply of magnesium, i.e., an RDA of 350–400 mg/day is recommended in pregnancy and of 310–360 mg/day during lactation, compared with 300–310 mg/day for non-pregnant or non-lactating women. Considering the 33% suboptimal serum Mg found in the German population [30], whether or not these amounts are really adequate should be verified.” (Fanni, et al., 2021)
Need for magnesium prenatally was described as doubled compared to a woman’s need when not pregnant, in a review on magnesium and bone health by Ciosek, et al., 2021.
Magnesium deficiency would add to the risk of tooth enamel demineralization by reducing immune function even more than it drops due to pregnancy alone and it reduces protein production which would affect salivary protein content. Saliva would be even less effective as an antimicrobial against cavity promoting species of bacteria. Reduced antibody production would be increasing risk of infection.
“Magnesium deficiency is associated with reduced protein synthesis, serum antibody titer, and decrease immune response [35].” (Fanni, et al., 2021)
Many lifestyle factors can increase risk of magnesium deficiency:
“Smokers have lower Mg levels in the femoral head and in the spongy bone of the femur than nonsmokers [11,42,48]. Changes in Mg concentrations in the body can also be caused by alcohol and coffee abuse, diet, stress, and in the course of some diseases, including heart failure, kidney diseases, atherosclerosis, neoplastic diseases, hypertension, diabetes, and postmenopausal osteoporosis [62,86,87]. Kuo et al. [46] found an influence of seafood consumption on the Mg bone content. A positive correlation between a diet containing seafood and the level of Mg in the bone was reported. Taking into account the bone diseases, Karaaslan et al. [53] reported a higher level of the element in the femoral neck of patients with osteoarthritis than patients with fractures. Additionally, Brodziak-Dopierała et al. [36] noted that patients with femoral neck fractures had lower Mg levels than subjects with degenerative changes. This could be related to the fact that there is a strong positive correlation between Ca and Mg in the mineralized tissues [88].”
Magnesium deficiency prenatally may lead to epigenetic changes during fetal development.
Magnesium deficiency prenatally can lead to epigenetic changes occurring in the fetus that affect the individual later in life. Magnesium deficiency would cause dysfunctional methylation cycles and disrupted methylation of genes.
“Experimental studies in mice evidenced that maternal Mg deficiency can result in behavioral deficits in the offspring during adult life, confirming a major role for an optimal magnesium status during pregnancy on the health status of newborns extending to adulthood [43].” […]
“At experimental level, the offspring of pregnant rats fed a low magnesium diet, showed hypermethylation in the hepatic 11β-hydroxysteroid dehydrogenase-2 promoter [49]. These data clearly indicate that magnesium deficiency during gestation may cause the epigenetic dysregulation of gene expression in the fetus, promoting different metabolic phenotypes in the newborn that might persist throughout life.” (Fanni, et al., 2021)
Magnesium is the smart choice for mom and baby - better magnesium status prenatally was associated with better cognitive skills in the children at age four.
“Very recently, the maternal magnesium status during gestation has been correlated with the cognitive outcomes of the neonates. To this end, magnesium serum levels were measured at 26–28 weeks of gestation and the cognitive development of the infants was evaluated at 4 years of age. Higher maternal magnesium serum levels were associated with higher scores in letters and writing identification, suggesting the existence of long-term influences of maternal magnesium on child’s cognitive development [55].” (Fanni, et al., 2021)
Being deficient in magnesium is more common in anyone with the standard diet and with the reduced mineral availability from glyphosate use. Pregnant and lactating women have a sizeable increase in their need for magnesium and it protects mom and baby in many ways.
Better oral health due to improved saliva immune response and a reduced risk of high blood sugar would be a bonus in addition to all the other benefits of magnesium adequacy.
“Trace elements, including magnesium, are an essential nutritional component for humans, particularly in the intrauterine life when fetal development occurs [56], and inadequate tissue concentrations of magnesium may have significant adverse effects on fetal weight at birth [52]. The need for magnesium increases during pregnancy, but the majority of pregnant women do not meet this increased need. Hypomagnesemia is frequently observed in pregnant women, both in developing and developed countries. Magnesium deficiency during pregnancy is associated with a higher health risk for both mother and newborn, including restricted fetal growth, intrauterine growth restriction, gestational diabetes, preterm labor, and pre-eclampsia.” […]
“The hypothesis that magnesium deficiency might be the basis of hyperreactivity of uterine muscle cells led to suggest magnesium supplementation during pregnancy as an optimal adjuvant therapy for the prevention of prematurity [47].
In a study focused on the possible influence of supplements on pregnancy outcome, in magnesium-supplemented pregnant mothers, the risk for neonates to undergo a low birth weight was significantly lower, as compared with mothers with no magnesium supplementation [58].” (Fanni, et al., 2021)
Magnesium adequacy in the mother is also safer for the newborn, premature babies in the following excerpt.
“In order to assess whether there is any relationship between antenatal magnesium dose and time of administration of therapy with intestinal injury in extreme preterms, 302 neonates born prematurely or with birth weight < 1000 g, whose mothers underwent magnesium sulfate supplementation during the last week before birth were followed-up. Antenatal magnesium sulfate exposure in extreme preterm newborns was not associated with an increased risk of necrotizing enterocolitis or of other intestinal injuries. On the contrary, necrotizing enterocolitis and spontaneous intestinal perforation were both decreased in the neonates of magnesium-supplemented mothers, in a dose-dependent manner, indicating a possible protective effect against NEC of magnesium maternal supplementation. Each 10 g increase in magnesium sulfate cumulative dose correlated with decrease in NEC death by 18.9% prior to discharge and by 21.9% during the first 2 weeks of life [78].” […]
“Antenatal magnesium sulfate administration reduced the risk of death or cerebral palsy and the inability to walk without assistance at 2 years of age [79].” (Fanni, et al., 2021)
Leg cramps are a common discomfort for many pregnant women and magnesium supplementation or an Epsom salt bath would help if magnesium is part of the need. If it doesn’t seem to help though, over-acidity throughout the body may also cause painful leg cramps. That could be an indicator that the saliva is also more acidic and is putting teeth at greater risk of demineralization.
“Oral administration of magnesium lowered the frequency and intensity of leg cramps in pregnant women, clearly indicating magnesium supplementation as a treatment of choice for pregnancy-induced leg cramps [82]. Conflicting results on the efficacy of magnesium supplementation in the therapy of leg cramps in pregnant women were reported in another meta-analysis [83], in which magnesium, taken orally by pregnant mothers for 2 to 4 weeks, did not significantly reduce the frequency and intensity of leg cramps compared with placebo or no treatment.” (Fanni, et al., 2021)
A very tiny amount of baking soda in a glass of water may help and not taste too yucky if over-acidity within the body is a cause of the leg cramps instead of the magnesium. Maybe try the Epsom salt soak first as Mg deficiency is a cause of muscle cramps, and then try the baking soda if it didn’t help enough. If the body doesn’t need a little boost of alkaline baking soda it will seem bad tasting in my own experience. The tongue can be good at telling what we need and how much. Tune in and learn to eat and drink “to taste” - to what tastes good at that particular time and place and state of health.
Another indicator of over-acidity within the body or diet is having a sudden urge to urinate and then only doing a tiny trickle that might even sting or burn a little (the acidity). When I was working and drinking a lot of coffee, I learned to have one mug of water in between each mug of coffee. And I started adding a dash of baking soda to my cup of coffee to offset the acidity. That added volume and took away the sting, but coffee is a diuretic. I was still visiting the restroom a lot. It just didn’t seem like a wasted effort (wtf is this? - overacidity).
Disclaimer: This information is being provided for educational purposes within the guidelines of Fair Use. While I am a Registered Dietitian this information is not intended to provide individual health guidance. Please see a health professional for individual health care purposes.
BowTiedGatorDDS’s Reference List
(Arima, et al., 2022) Arima H, Calliope AS, Fukuda H, Nzaramba T, Mukakarake MG, Wada T, Yorifuji T, Mutesa L, Yamamoto T. Oral cleaning habits and the copy number of periodontal bacteria in pregnant women and its correlation with birth outcomes: an epidemiological study in Mibilizi, Rwanda. BMC Oral Health. 2022 Sep 26;22(1):428. doi: 10.1186/s12903-022-02443-4. PMID: 36163018; PMCID: PMC9512986. https://pubmed.ncbi.nlm.nih.gov/36163018/ / Fulltext: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9512986/
(Hartzer, 1969) Hartzer, R.C., Immune Reactions in the Gingiva of the Pregnant and Non-Pregnant Human Female, Master’s Thesis, Loyala University, Chicago, 1969, https://ecommons.luc.edu/cgi/viewcontent.cgi?article=3367&context=luc_theses
(Herring, et al., 2018) Herring CM, Bazer FW, Johnson GA, Wu G. Impacts of maternal dietary protein intake on fetal survival, growth, and development. Exp Biol Med (Maywood). 2018 Mar;243(6):525-533. doi: 10.1177/1535370218758275. Epub 2018 Feb 22. PMID: 29466875; PMCID: PMC5882021. https://ncbi.nlm.nih.gov/pmc/articles/PMC5882021/
(Pitkin, 1975) Pitkin RM. Calcium metabolism in pregnancy: a review. Am J Obstet Gynecol. 1975 Mar 1;121(5):724-37. doi: 10.1016/0002-9378(75)90481-0. PMID: 1090175. https://pubmed.ncbi.nlm.nih.gov/1090175/
(Wu, Chen, Jiang, 2015) Wu M, Chen SW, Jiang SY. Relationship between gingival inflammation and pregnancy. Mediators Inflamm. 2015;2015:623427. doi: 10.1155/2015/623427. Epub 2015 Mar 22. PMID: 25873767; PMCID: PMC4385665. https://ncbi.nlm.nih.gov/pmc/articles/PMC4385665/
(Yousefi, Parvaie, Riahi, 2020) Yousefi M, Parvaie P, Riahi SM. Salivary factors related to caries in pregnancy: A systematic review and meta-analysis. J Am Dent Assoc. 2020 Aug;151(8):576-588.e4. doi: 10.1016/j.aime.2020.04.021. PMID: 32718487. https://pubmed.ncbi.nlm.nih.gov/32718487/ *paywall
My Reference List
(Abou-Neel, et al., 2016) Abou Neel EA, Aljabo A, Strange A, Ibrahim S, Coathup M, Young AM, Bozec L, Mudera V. Demineralization-remineralization dynamics in teeth and bone. Int J Nanomedicine. 2016 Sep 19;11:4743-4763. doi: 10.2147/IJN.S107624. PMID: 27695330; PMCID: PMC5034904. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5034904/
(Arendt-Nielsen, et al., 2022) Lars Arendt-Nielsen, PhD and others, The Role of TRP Channels in Nicotinic Provoked Pain and Irritation from the Oral Cavity and Throat: Translating Animal Data to Humans, Nicotine & Tobacco Research, Volume 24, Issue 12, December 2022, Pages 1849–1860, https://doi.org/10.1093/ntr/ntac054 https://academic.oup.com/ntr/article/24/12/1849/6535530
(CC BY-NC-ND 4.0, Bhatia, Shatanof, Bordoni, 2023) Bhatia, A., Shatanof, R.A., Bordoni, B., Embryology, Gastrointestinal, Last update May 2023 (CC BY-NC-ND 4.0) (http://creativecommons.org/licenses/by-nc-nd/4.0/ ) https://www.ncbi.nlm.nih.gov/books/NBK537172/
(Brouns, 2021) Brouns F. Phytic Acid and Whole Grains for Health Controversy. Nutrients. 2021 Dec 22;14(1):25. doi: 10.3390/nu14010025. PMID: 35010899; PMCID: PMC8746346. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8746346/
(caortho.org) California Assoc. of Orthodontists, How Braces Work, Aug 27, 2019, https://caortho.org/how-braces-work/
(Cappadone, et al., 2021) Cappadone C, Malucelli E, Zini M, Farruggia G, Picone G, Gianoncelli A, Notargiacomo A, Fratini M, Pignatti C, Iotti S, Stefanelli C. Assessment and Imaging of Intracellular Magnesium in SaOS-2 Osteosarcoma Cells and Its Role in Proliferation. Nutrients. 2021 Apr 20;13(4):1376. doi: 10.3390/nu13041376. PMID: 33923895; PMCID: PMC8073505. https://doi.org/10.3390/nu13041376 https://www.mdpi.com/2072-6643/13/4/1376
(Castiglioni, et al., 2013) Castiglioni S, Cazzaniga A, Albisetti W, Maier JA. Magnesium and osteoporosis: current state of knowledge and future research directions. Nutrients. 2013 Jul 31;5(8):3022-33. doi: 10.3390/nu5083022. PMID: 23912329; PMCID: PMC3775240. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3775240/
(Chen, et al., 2015) Chen H, Iinuma M, Onozuka M, Kubo KY. Chewing Maintains Hippocampus-Dependent Cognitive Function. Int J Med Sci. 2015 Jun 9;12(6):502-9. doi: 10.7150/ijms.11911. PMID: 26078711; PMCID: PMC4466515. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4466515/
(Ciosek, et al., 2021) Ciosek Ż, Kot K, Kosik-Bogacka D, Łanocha-Arendarczyk N, Rotter I. The Effects of Calcium, Magnesium, Phosphorus, Fluoride, and Lead on Bone Tissue. Biomolecules. 2021 Mar 28;11(4):506. doi: 10.3390/biom11040506. PMID: 33800689; PMCID: PMC8066206. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8066206/
(Duverger Beniash, Morasso 2016) Duverger O, Beniash E, Morasso MI. Keratins as components of the enamel organic matrix. Matrix Biol. 2016 May-Jul;52-54:260-265. doi: 10.1016/j.matbio.2015.12.007. Epub 2015 Dec 17. PMID: 26709044; PMCID: PMC4875797. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4875797/
(Fanni, et al., 2021) Fanni, D., Gerosa, C., Nurchi, V.M. et al. The Role of Magnesium in Pregnancy and in Fetal Programming of Adult Diseases. Biol Trace Elem Res 199;3647–3657 (2021). https://doi.org/10.1007/s12011-020-02513-0 https://link.springer.com/article/10.1007/s12011-020-02513-0
(glosciencepro.com) Glo Science Professional, Are Teeth Made Of Keratin? July 23, 2022, glosciencepro.com, https://glosciencepro.com/blogs/teeth-whitening/what-are-teeth-made-of-and-their-similarities-to-hair
(Thangamani, 2017) Thangamani, Dr. Carrie, Complications with Braces, chtortho.com, Jan 27, 2017 https://chtortho.com/complications-with-braces/
(Harvard.edu, 2014), Vitamin A and Your Bones, health.harvard.edu, March 9, 2014, https://www.health.harvard.edu/newsletter_article/vitamin-a-and-your-bones
(Houghton, et al., 2020) Houghton JW, Carpenter G, Hans J, Pesaro M, Lynham S, Proctor G. Agonists of Orally Expressed TRP Channels Stimulate Salivary Secretion and Modify the Salivary Proteome. Mol Cell Proteomics. 2020 Oct;19(10):1664-1676. doi: 10.1074/mcp.RA120.002174. Epub 2020 Jul 10. PMID: 32651226; PMCID: PMC8014997. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8014997/
(Johansson, Ericson, 1987) Johansson I, Ericson T. Saliva composition and caries development during protein deficiency and beta-receptor stimulation or inhibition. J Oral Pathol. 1987 Mar;16(3):145-9. doi: 10.1111/j.1600-0714.1987.tb01482.x. PMID: 3040946. https://pubmed.ncbi.nlm.nih.gov/3040946/
(Kim/Skeleton) Kim’s Body Breakdown, Skeletal system, home.adelphi.edu, https://home.adelphi.edu/~ki20971/skeletal.html
(Kote, Kote, Nagesh, 2011) Kote S, Kote S, Nagesh L. Effect of pomegranate juice on dental plaque microorganisms (streptococci and lactobacilli). Anc Sci Life. 2011 Oct;31(2):49-51. PMID: 23284205; PMCID: PMC3530267. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3530267/
(Lasisi, Alada, 2015) Lasisi TJ, Alada AR. Effects of induced-kwashiorkor on salivary parameters in Wistar rats. Afr J Med Med Sci. 2015 Jun;44(2):125-32. PMID: 26937525. https://pubmed.ncbi.nlm.nih.gov/26937525/
(Meyer, et al., 2022) Meyer, F., Enax, J., Amaechi, B.T., Limeback, H., Fabritius, H.-O., Ganss, B., et al., Hydroxyapatite as Remineralization Agent for Children's Dental Care, Front. Dent. Med, 25 April 2022, Sec. Pediatric Dentistry, Volume 3 - 2022 | https://doi.org/10.3389/fdmed.2022.859560 https://www.frontiersin.org/articles/10.3389/fdmed.2022.859560/full
(Milagros, et al., 2005) Milagros G. Huerta, James N. Roemmich, Marit L. Kington, Viktor E. Bovbjerg, Arthur L. Weltman, Viola F. Holmes, James T. Patrie, Alan D. Rogol, Jerry L. Nadler; Magnesium Deficiency Is Associated With Insulin Resistance in Obese Children. Diabetes Care 1 May 2005; 28 (5): 1175–1181. https://doi.org/10.2337/diacare.28.5.1175 https://diabetesjournals.org/care/article/28/5/1175/27632/Magnesium-Deficiency-Is-Associated-With-Insulin
(Moldenhauer, et al., 2022) LM, Hull ML, Foyle KL, McCormack CD, Robertson SA. Immune-Metabolic Interactions and T Cell Tolerance in Pregnancy. J Immunol. 2022 Oct 15;209(8):1426-1436. doi: 10.4049/jimmunol.2200362. PMID: 36192117. https://pubmed.ncbi.nlm.nih.gov/36192117/
(Morkmued, et al., 2017) Morkmued, S., Laugel-Haushalter, V., Mathieu,E., Schuhbaur, B., Hemmerlé, J., Dollé, P., et al., Retinoic Acid Excess Impairs Amelogenesis Inducing Enamel Defects, Front. Physiol., 06 January 2017, Sec. Craniofacial Biology and Dental Research, Vol 7, 2016, https://doi.org/10.3389/fphys.2016.00673 https://www.frontiersin.org/articles/10.3389/fphys.2016.00673/full
(Nadler, et al., 1993) Nadler JL, Buchanan T, Natarajan R, Antonipillai I, Bergman R, Rude R. Magnesium deficiency produces insulin resistance and increased thromboxane synthesis. Hypertension. 1993 Jun;21(6 Pt 2):1024-9. doi: 10.1161/01.hyp.21.6.1024. PMID: 8505087. https://www.ahajournals.org/doi/epdf/10.1161/01.HYP.21.6.1024
(news-medical.net) Risks of Dental Braces, news-medical.net, https://www.news-medical.net/health/Risks-of-Dental-Braces.aspx
(O’Hagan-Wong, et al., 2022) O'Hagan-Wong K, Enax J, Meyer F, Ganss B. The use of hydroxyapatite toothpaste to prevent dental caries. Odontology. 2022 Apr;110(2):223-230. doi: 10.1007/s10266-021-00675-4. Epub 2021 Nov 22. PMID: 34807345; PMCID: PMC8930857. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8930857/
(Pitkin, 1985) Pitkin RM. Calcium metabolism in pregnancy and the perinatal period: a review. Am J Obstet Gynecol. 1985 Jan 1;151(1):99-109. doi: 10.1016/0002-9378(85)90434-x. PMID: 3881031. https://pubmed.ncbi.nlm.nih.gov/3881031/ *paywall
(Pujol, et al., 2023) Pujol A, Sanchis P, Grases F, Masmiquel L. Phytate Intake, Health and Disease: "Let Thy Food Be Thy Medicine and Medicine Be Thy Food". Antioxidants (Basel). 2023 Jan 7;12(1):146. doi: 10.3390/antiox12010146. PMID: 36671007; PMCID: PMC9855079. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9855079/
(ref1) Ten Steps to Create a BowTied Animal, bowtiedchukar.com, https://bowtiedchukar.com/ten-steps-to-create-a-bowtied-animal/
(ref2) BowTied Bull, BowTiedBull FAQ - Will Be Updated Over Time, bowtiedbull.substack.com, May 3, 2021, https://bowtiedbull.substack.com/p/bowtiedbull-faq-will-be-updated-over?utm_source=bowtiedchukar.com&utm_medium=referral&utm_campaign=steps_to_create_a_bowtied_animal
(Rondanelli, et al., 2021) Rondanelli, M., Faliva, M.A., Tartara, A. et al. An update on magnesium and bone health. Biometals 34;715–736 (2021). https://doi.org/10.1007/s10534-021-00305-0 https://link.springer.com/article/10.1007/s10534-021-00305-0
(Schlemmer, et al., 2009) Schlemmer U, Frølich W, Prieto RM, Grases F. Phytate in foods and significance for humans: food sources, intake, processing, bioavailability, protective role and analysis. Mol Nutr Food Res. 2009 Sep;53 Suppl 2:S330-75. https://onlinelibrary.wiley.com/doi/abs/10.1002/mnfr.200900099
(Shaila, Pai, Shetty, 2013) Shaila M, Pai GP, Shetty P. Salivary protein concentration, flow rate, buffer capacity and pH estimation: A comparative study among young and elderly subjects, both normal and with gingivitis and periodontitis. J Indian Soc Periodontol. 2013 Jan;17(1):42-6. doi: 10.4103/0972-124X.107473. PMID: 23633771; PMCID: PMC3636943. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3636943/
(Sun Oaks Dental) Sun Oaks Dental, Insulin Resistance is a Risk Factor for Perio Disease, sunoaksdental.com, Nov 16, 2016, https://www.sunoaksdental.com/insulin-resistance-is-a-risk-factor-for-perio-disease
(Tebben, Singh, Kumar, 2016) Tebben PJ, Singh RJ, Kumar R. Vitamin D-Mediated Hypercalcemia: Mechanisms, Diagnosis, and Treatment. Endocr Rev. 2016 Oct;37(5):521-547. doi: 10.1210/er.2016-1070. Epub 2016 Sep 2. PMID: 27588937; PMCID: PMC5045493. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5045493/
(Törmä, 2011) Törmä H. Regulation of keratin expression by retinoids. Dermatoendocrinol. 2011 Jul;3(3):136-40. doi: 10.4161/derm.3.3.15026. Epub 2011 Jul 1. PMID: 22110773; PMCID: PMC3219164. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3219164/
(Umar, et al., 2016) Umar D, Dilshad B, Farhan M, Ali A, Baroudi K. The effect of pomegranate mouthrinse on Streptococcus mutans count and salivary pH: An in vivo study. J Adv Pharm Technol Res. 2016 Jan-Mar;7(1):13-6. doi: 10.4103/2231-4040.173266. PMID: 26955605; PMCID: PMC4759979. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4759979/
(Uwitonze, et al., 2020) Uwitonze, A.M., Rahman, S., Ojeh, N., Grant, W.B., Kaur, H., Haq, A., Razzaque, M.S., Oral manifestations of magnesium and vitamin D inadequacy, The Journal of Steroid Biochemistry and Molecular Biology, Vol 200, 2020, 105636, ISSN 0960-0760, https://doi.org/10.1016/j.jsbmb.2020.105636. https://www.sciencedirect.com/science/article/pii/S0960076019301815 *paywall
(van Driel, van Leeuwen, 2023) van Driel M, van Leeuwen JPTM. Vitamin D and Bone: A Story of Endocrine and Auto/Paracrine Action in Osteoblasts. Nutrients. 2023; 15(3):480. https://doi.org/10.3390/nu15030480 https://www.mdpi.com/2072-6643/15/3/480
(Xiao Dental) Xiao Dental, Hormones Happen: Why Women Are More Prone to Cavities, March 18, 2014, winning-smiles.com https://www.winning-smiles.com/healthtopics2/2014/3/18/hormones-happen-why-women-are-more-prone-to-cavities.html
So sorry to hear that your dad passed on Sunday Jennifer. May he rest in peace.
Very happy you wrote this article today, filled with important health information that I didn't know. (I turned 65 on Sunday. Trying to hang on to my remaining teeth...)
Thank you. 💖
Tooth “hygiene” is way overrated. No other mammal brushes their teeth to prevent dental decay.