



Round two - Retinoid Toxicity & CoV, by another research team.
Follow up to the last post, still reading but I am passing forward a relevant hypothesis article I found yesterday - CoV pathogenesis & lack of Retinoid signaling by vitamin A and D.

Last post: SPED meets Retinoid Toxicity - Round One. This post contains Excerpts and Figures from “A novel hypothesis for COVID-19 pathogenesis: Retinol depletion and retinoid signaling disorder.” The team is suggesting that the SARS-CoV-2 infection leads to a severe depletion of vitamin A which then further increases the hyperinflammatory response.
This situation may be more complex as the vitamin A is converted into Retinoic Acid, there may be an excess of the activated form in addition to the lack of the inactive form, or the illness may have phases, acute infection and lingering LongCovid/ME/CFS. More on that later - first the hypothesis excerpts and -
Two related boxes from a Table that I am still working on:
Regarding Histamine Excess effects: It causes increased IL-6 and NF-kB. (Park, et al, 2014)
Regarding Retinoid Toxicity effects: It may cause changes in the balance of inactive to active forms of vitamin A and the resulting deficiency of Vitamin A increases NF-kB because it is needed to form Activated Retinoic Acid (ATRA) which can inhibit the creation of NF-kB and IL-6. (Austenaa et al, 2004) Inflammation will lead to depletion of retinol as it is converted to Retinoic Acid to help reduce the inflammation and then deficiency of the inactive retinol (vitamin A) will lead to increased NF-kB and increased inflammation again. (Sarohan et al, 2021)
During infection the standard nutrient recommendations are not applicable because those specifically are for “healthy” people. During infection we need extra vitamin A, Bs, C, D, and trace minerals like magnesium, selenium, iodine, and manganese* (*in tiny amounts).
“A novel hypothesis for COVID-19 pathogenesis: Retinol depletion and retinoid signaling disorder.”“Highlights” (Sarohan et al, 2021)
•"Retinoid signaling plays a central role in the pathogenesis of COVID-19. Both vitamin A and vitamin D employ retinoid signaling.
• A proper retinoid signaling establishes a balance between regulatory T cells and pro-inflammatory Th17 cells.
• Dysregulated retinoid signaling suppresses Tregs and favors development of hyperinflammatory Th17 in COVID-19.
• COVID-19 infection rapidly consumes body’s retinol leading to dysregulated retinoid signaling and hyperinflammation.
• This causes cytokine storm leading to multi-organ system involvement.” (Sarohan et al, 2021)

Figure 1. shows on the left that retinol is needed to form Retinoic Acid (RA) and all-trans Retinoic Acid (ATRA) and 9-cis Retinoic Acid in order to activate the gene transcription by the Retinoic Acid Receptor (RAR) and the RXR retinoid receptor in order to form Retinoid Inducible-1 (RIG-1) - in the blue box. RIG-1 is needed to form interferon (IFN) in the green box in the middle. Lack of Interferon would then be a result of deficiency of vitamin A needed to form ATRA and 9-cisRA.
Interferons are formed in response to viral RNA signals. Vitamin A is part of our front-line defense against virus. Severity of measles is worse with vitamin A deficiency.
The third column of Figure 1 shows how retinol deficiency would lead to a lack of Retinoic Acid (RA) which can inhibit ( - - -I ) several areas of the inflammatory pathways that lead to production of NF-kB. (Sarohan et al, 2021)
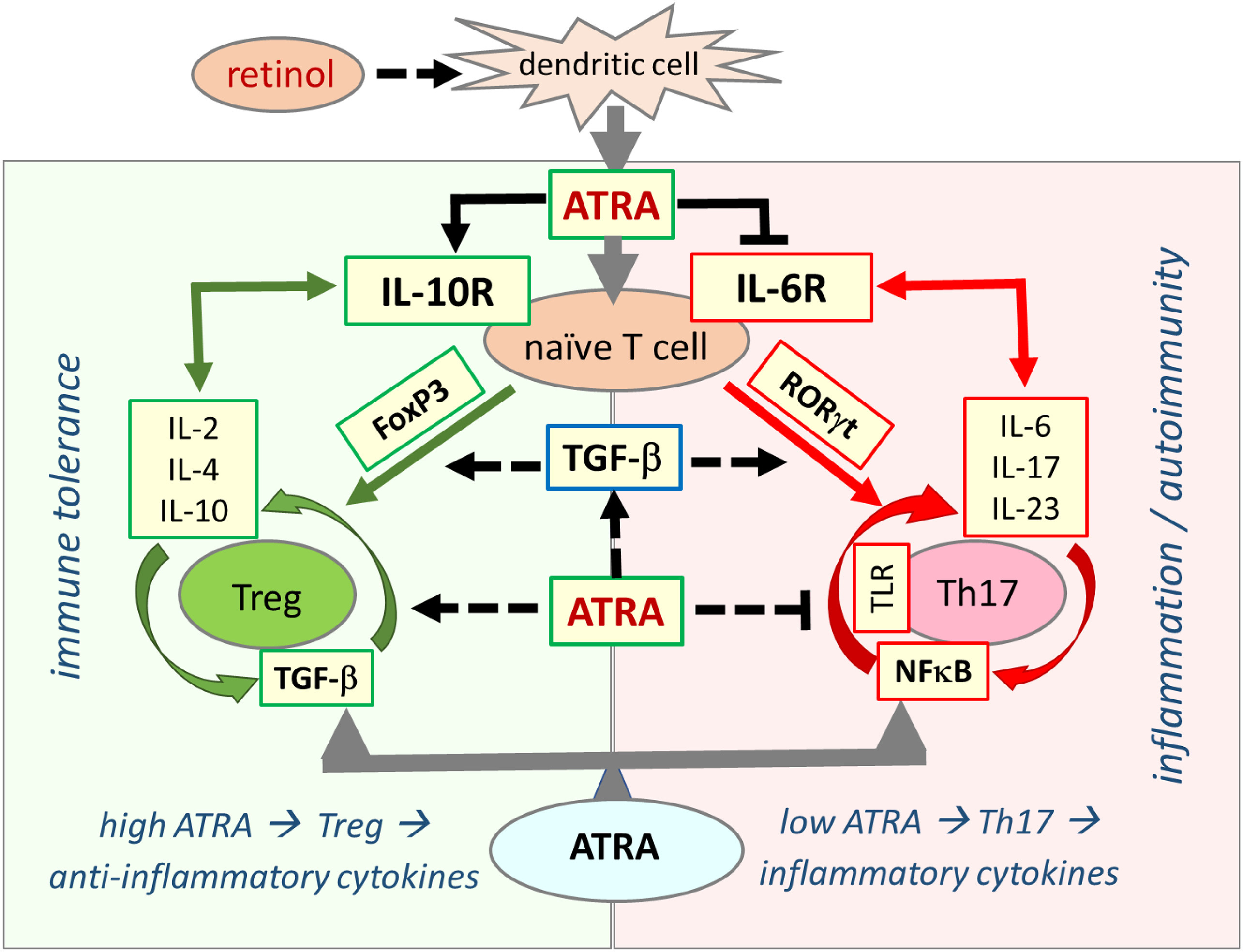
Figure 2 shows how having plenty of all-trans Retinoic Acid (ATRA) helps promote TReg cells and anti-inflammatory cytokines which help prevent autoimmune reactions. And lack of ATRA leads to increased production of Th17 cells which are more prevalent in autoimmune disease, and it leads to more inflammatory cytokines. The ATRA would have inhibited production of IL-6R and further cytokine production.
Maybe there are two phases? Acute and LongCovid / ME/CFS?
My initial thoughts: The SARS-CoV-2 pathology may have phases - in the acute illness providing adequate vitamin A is likely a need and protective, while for some LongCovid or jab injured people with long-term symptoms the liver gene change seen with the Epstein-Barr Virus (DHRS9, (Jones, et al, 2007)) may have occurred which would then make intake of larger amounts of vitamin A into an ongoing risk rather than fully a benefit.
If in a chronic latent infection, the virus was able to promote more differentiation of endothelial cells for it to then infect by inducing activation of more Retinoic Acid, then the other symptoms of Retinoid Toxicity might also be occurring as the normal control for not over-activating too much Retinoic acid seems to be absent in the people with ME/CFS. So, they would be chronically low in retinol - which would be inflammatory - promoting NF-kB, and they would have excess active Retinoic Acid, which can also be inflammatory in excess. Cytokine panels for people with ME/CFS tend to a mixture of anti-inflammatory and inflammatory. Excess Retinoic Acid can cause a lot of varied actions as it impacts gene transcription of many thousands of protein types.
For people like me, who went into the initial CoV infection with a history of ME/CFS type symptoms and possibly an EBV infection in the past, just the right amount of vitamin A would likely be needed. Mega doses might be over-converted into too much Retinoic Acid. When I was ill with CoV in March 2020 I wasn’t aware of the Retinoid Toxicity problem that I had had for decades already. I was eating carrots, kale, sweet potatoes and apricots etc, most days at least one or two excellent sources. I learned of Retinoid Toxicity and the EBV history in the autumn of 2020 after I had been eating lots and lots of mangos in addition to my daily carrot and kale habit. That level of daily super-rich carotenoid sources had led to non-healing skin symptoms, so I started reading more widely. Retinoid Toxicity Survey (transcendingsquare.com)
My diet at that time already was lower in vitamin A than a standard diet because I had to stop eating all animal products during an earlier autoimmune flair-up that I traced to albumin antibodies seemingly. Excess vitamin A might have been a factor in my symptoms at that time too as not eating meat or dairy would reduce intake of the retinol form of vitamin A.
Another excerpt:
“With the depletion of retinol and disrupted RA signaling, which may be the case in severe COVID-19, the transformation of naïve T cells to regular T cells is blocked, while transformation into effector Th17 cells is promoted [34], [35], [36]. As a result, excessive cytokine release and systemic organ damage may occur. Meanwhile, the cellular and mitochondrial DNA fragments emanating from dying host cells and RNA fragments emanating from fragmented viral particles will continue to activate the inflammatory NF-κB (nuclear factor kappa light chain enhancer of activated B cells) signaling cascade through TLR [37]. The continuous and intense stimulation of TLR causes hyperactivation of NF-κB pathway and excessive stimulation of the immune cells resulting in excessive cytokine discharge and reprogramming of B and T cell development that ultimately leads to devastating systemic effects seen in COVD-19 [38], [39], [40], [41].” (Sarohan et al, 2021)
No matter what else is going on - Nrf2 promoters are needed in quantity, several times a day, in order to help balance the excess NF-kB response. It directly inhibits Nrf2 activity because they share a Clock protein - two shifts of workers are active in our body and modern life, too often, is keeping the day shift on board 24/7. Nrf2 is our growth and repair, night-time shift. Melatonin supplements throughout the day seem protective and I use an eye cover when napping or sleeping. I had light sensitivity symptoms while sick with CoV and napped quite a bit the first week of symptom onset. See this post for self care tips for reducing the hyperinflammatory signaling from modern life, and/or an infection.
My goal in learning and sharing info, is both protection of my personal health and help for public health - those who are interested in self-care options. My genetic differences and autoimmune history placed me in the high-risk category for more severe CoV symptoms. As a human subject in this open-air passive “vaccination” experiment I have been maintaining or restoring my health, with some difficulty, rather than worsening into more severe categories of illness. It isn’t “easy”, but severe illness is not easy either.
Why are both vitamin A deficiency and Retinoid excess so bad for us? because retinoid signaling impacts almost everything else in our body. The Table that I am working on shows how histamine excess and Retinoid Toxicity have very similar long-term risks, including liver and kidney damage, but are not quite the same. Retinoid Toxicity would be causing histamine excess and also other problems too.
“Due to the widespread distribution and intensive activity of retinoid signaling in various organ systems, impairment in retinoid signaling affects almost all organ systems [42], [43], [44], [45]. Likewise, COVID-19 presents very common and similar various symptoms, clinical findings, and multi-organ involvement [36], [46], [47]. Damaged liver may lose retinol reserves faster [22] causing retinoid signaling impairment that may lead to the emergence of severe clinical pictures, multiple organ injuries, and chronic post-COVID syndromes [48], [49], [50].” (Sarohan et al, 2021)
Whatever is going on currently, is not very safe or effective at protecting human health. Consumers be wary.
Addition - What does NF-kB do? Helps us fight infections, is a response to anything that causes oxidative stress -
“In immune cells, NF-κB proteins regulate immune cell development, activation, survival, and cytokine production [200], [201]. NF-κB proteins are activated through stimulants such as cytokines, stress, free radicals, ultraviolet radiation,* and infections [200]. They play a central role in regulating immune response to infections. They are highly active in inflammatory diseases and control transcription of many genes involved in immune response and cytokine production [200], [201].” (Sarohan et al, 2021)
*Sunburn Pox!
and another gene that is upregulated in patients with more severe illness from CoV:
“A recent large scale, multicenter, multi-tissue genetically regulated gene expression profiling study have identified high IL-10 receptor beta (IL10RB) expression as the key regulator of COVID susceptibility and severity [141]. This study showed that IL10RB is significantly upregulated in individuals susceptible to COVID-19 hospitalization and downregulated in non-hospitalized infected individuals. Therefore, IL10RB expression level was found to be the best prediction of the worst COVID-19 outcome. The same study also demonstrated 10–100 times increased expression of some pathway markers including dendritic cell migration, chemokine and cytokine receptor signaling, and inflammatory response, in severe COVID-19 cases and found that retinol and immunosuppressant drug Azothioprine are significantly associated with strong decrease of COVID-19 infection [141].” (Sarohan et al, 2021)
Gene alleles for the Interleukon 10 receptor beta type are seen in more severe HIV and may be more common in African Americans.
Interleukin-10 (IL-10) Pathway: Genetic Variants and Outcomes of HIV-1 Infection in African American Adolescents - PMC (nih.gov)
More notes - a biphasic aspect to COVID19 is described in section 6.5. The initial viral response has normal interferon production and then in more severe stages the shift to Th17 cells from the protective Treg cells is seen. The research team suggest that at that stage the body stores of retinol and retinoic acid have been depleted.
“Host immune cells recognize self-DNA fragments in autoimmune diseases such as lupus, psoriasis, arthritis, and multiple sclerosis [38], [228], [267], [276], [277], [278], [279], [280]. In COVID-19, autoimmune pathogenesis proceeds with the severe inflammatory process that develops due to dysregulation between Treg and Th17 cells [126], [258], [261], [262]. This autoimmune response in COVID-19 may well be caused, at least partially, by the dysregulation and loss of self-tolerance in the immune system that develops most likely as a result of retinol depletion and retinoid signaling disorders. The decrease in Treg cell numbers due to the low levels of retinol and ATRA in COVID-19 can lead to a breakdown of immune tolerance and development of autoimmune pathogenesis [233], [236], [281].” (Sarohan et al, 2021)
Adequate vitamin A in advance would also be helping with the nasal defense - stop the SARS infection before it gets to the lungs where it is harder for the body’s defenses to stop the infection.
“VitA and its derivatives provide their main protective effects against viral infections through upregulating Type I IFN synthesis [51]. They also strengthen the mucosal immunity by increasing secretory IgA production and mucosal barrier formation [288], [299]. In the case of COVID-19, Riva et al., have reported that the expression of genes within RAR signaling pathway were significantly decreased in Vero E6 culture cells infected with SARS-CoV-2 [140]. They further found that RA receptor agonists inhibited SARS-CoV-2 replication, and that this inhibition was reversed with RA receptor antagonist molecules indicating the importance of RA receptor signaling in COVID-19 pathogenesis [140]. These data demonstrate that retinol metabolism and retinoid signaling can function as a critical host-pathogen-interaction circuit in controlling SARS-CoV-2 infection, which indicates that VitA supplementation may help fight COVID-19 [41], [59], [303].” (Sarohan et al, 2021)
Disclaimer: This information is being shared within the guidelines of Fair Use for educational purposes and is not intended to provide individual health care guidance. Please seek a functional health care practitioner for individualized health guidance.
Reference List
(Jones, et al, 2007) Jones RJ, Dickerson S, Bhende PM, Delecluse HJ, Kenney SC. Epstein-Barr virus lytic infection induces retinoic acid-responsive genes through induction of a retinol-metabolizing enzyme, DHRS9. J Biol Chem. 2007 Mar 16;282(11):8317-24. doi: 10.1074/jbc.M608667200. Epub 2007 Jan 22. PMID: 17244623. https://www.jbc.org/content/282/11/8317.long
(Park et al, 2014) Park IH, Um JY, Cho JS, Lee SH, Lee SH, Lee HM. Histamine Promotes the Release of Interleukin-6 via the H1R/p38 and NF-κB Pathways in Nasal Fibroblasts. Allergy Asthma Immunol Res. 2014 Nov;6(6):567-72. doi: 10.4168/aair.2014.6.6.567. Epub 2014 Jul 28. PMID: 25374757; PMCID: PMC4214978. https://pubmed.ncbi.nlm.nih.gov/25374757/
(Sarohan et al, 2021) Sarohan AR, Kizil M, Inkaya AC, et al., (2021). A novel hypothesis for COVID-19 pathogenesis: Retinol depletion and retinoid signaling disorder. Cellular Signalling 87 (2021) https://www.sciencedirect.com/science/article/pii/S0898656821002102?via%3Dihub
(Shrestha et al., 2010) Shrestha S, Wiener HW, Aissani B, Song W, Shendre A, Wilson CM, Kaslow RA, Tang J. Interleukin-10 (IL-10) pathway: genetic variants and outcomes of HIV-1 infection in African American adolescents. PLoS One. 2010 Oct 14;5(10):e13384. doi: 10.1371/journal.pone.0013384. PMID: 20976276; PMCID: PMC2954785. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2954785/
This article is a little over my pay grade. But since around April of 2020 I have read so many technical articles like yours. I currently take between 1,000-1500 mcg of Vit A per day. I’m a little confused as to what dose to take if I ever contract Covid. I am unjabbed also. I currently follow the FLCCC guidelines ( and others) to boost my immune system. Thank you for what you are doing🌹